

INTRODUCTION
Physical inactivity is a global health crisis of the 21st century. The World Health Organization reports that each year physical inactivity will cost the lives of approximately 3.2 million people worldwide [1], making it the fourth leading cause of mortality [2]. Physical inactivity also increases morbidity, as it is strongly related to an increased risk of obesity2, as well as several non-communicable diseases, such as cardiovascular disease, type 2 diabetes, osteoporosis, and certain types of cancer [3]. Physical inactivity has also been associated with the development of mental health disorders [4], as well as decreased emotional well-being [5] and reduced quality of life [6]. Although most of the ill effects related to physical inactivity manifest in adulthood, the development of these problems begins much earlier. Adolescence is when individuals establish many of their lifestyle choices, and as such interventions addressing physical inactivity should target adolescence for establishing healthy lifestyle habits.
Physical literacy is defined as the motivation, confidence, physical competence, knowledge and understanding to value and engage in physical activity (PA) throughout life [7]. Thus, physical literacy provides the build blocks for a healthy, active lifestyle. Canadian Physical Activity Guidelines recommend children and youth accumulate 60 minutes of moderate-to-vigorous PA per day when averaged across a week [8]. Despite the health risks associated with physical inactivity, currently only 1/3 of healthy Canadian children meet these guidelines [9]. Recent evidence has shown that PA levels begin to decline at 7 years of age [10], with the decline continuing throughout childhood and adolescence. Of particular concern, this decline becomes even more rapid and pronounced during adolescence [11]. In Canada, 48% of children 5 to 11 meet the PA guideline, but this proportion decreases to 24% among adolescents 12 to 17 years of age [9]. Physical inactivity in childhood and adolescence has been associated with obesity [12], decreased self-esteem [13], and delayed motor skill development [14]. PA behaviour in youth has also been shown to track into adulthood [15]. Thus, the lack of PA in youth will have immediate and long-term health effects (e.g., high blood pressure, obesity, metabolic syndrome, and poor bone density) [16].
To address the decrease in PA during adolescence, the YMCA-YWCA of the National Capital Region developed a program called the Y Kids Academy. The program targeted youth in grade 6, primarily 11 to 12 years of age. The Y Kids Academy was designed to improve PA and healthy lifestyle knowledge and enable participants to safely engage in fitness training. Conditioning equipment at YMCA-YWCA facilities is typically restricted to adolescents and adults. It was hypothesized that enabling access to the conditioning areas for personal training would be perceived as an incentive as by the pre-adolescent youth participants. Youth who successfully complete the Y Kids Academy receive a complimentary 1-year membership to all YMCA-YWCA of the National Capital Region facilities.
The primary goal of this study was two-fold. First, we sought to evaluate whether the program would successfully attract participants with lower levels of physical literacy. Second, we sought to identify whether the Y Kids Academy Student Questionnaire accurately reflected the physical literacy knowledge of participants (i.e., validity of the questionnaire developed for the Y Kids Academy). The secondary aims of this study were to assess whether participation in the Y Kids Academy program would increase the healthy living knowledge of youth participants, change parent perceptions of the participant’s healthy living behaviours or change the family environment to support healthier lifestyles. We hypothesized that the complimentary membership would preferentially attract adolescents who were already active and that the questionnaire would accurately reflect the physical literacy knowledge of the participants. Furthermore, we hypothesized that participation in the program would increase healthy living knowledge among participants, improve parent perceptions of their child’s physical activity behaviours and impact the family environment and healthy living practices.
METHODS AND MATERIALS
The cross-sectional research protocol to evaluate the Y Kids Academy was approved by the Research Ethics Board at the Children’s Hospital of Eastern Ontario (CHEO IRB/REB #13/203X). Data collection occurred from 2014-2015 in conjunction with Y Kids Academy program offerings. Written parent informed consent and youth verbal assent were required for study participation. The evaluation of the Y Kids Academy included two assessment sessions, before and after the youth attended the Y Kids Academy. Before attending the Y Kids Academy, participants completed a standardized assessment of physical literacy and a questionnaire assessing their knowledge of healthy living. Parents were also given a questionnaire to assess their perceptions of their children’s PA and healthy living behaviours. After the completion of Y Kids Academy participation, the same youth and parent questionnaires were completed. The first and second assessments were either within the same week or one month apart, depending on whether the child was enrolled in a summer camp or community format, respectively.
Y Kids Academy Program Overview
The Y Kids Academy (http://www.ymcaywca.ca/Children/healthfitness/kidsacademy) was designed to enhance knowledge and understanding of PA and healthy living among youth. It was created in response to the 2013 Active Healthy Kids Canada Report, which indicated that only 7% of children 5 to 11 years of age and 4% of youth 12 to 17 years of age were achieving the guidelines at that time, which recommended 60 minutes of moderate-to-vigorous PA be performed every day (in contrast to the current recommendations of an average of 60 minutes per day) [17]. Specific objectives of the program included the development of confidence and competence for cardiovascular, muscular and flexibility activities, the generation of more positive attitudes and behaviours for healthy living, and the removal of barriers for young adolescent participation in exercise programs and access to facilities while exposing families to the YMCA-YWCA and its programming.
The program was initially offered in 2014 and 2015 as an after school, evening or weekend class (i.e., community format) at four YMCA-YWCA centres across the National Capital Region (pseudonyms used in this report for these locations are Russel, Timothy, Ranger, and Camble). The community format of the Y Kids Academy consisted of eight 1.5 hour sessions delivered twice per week for four weeks. Each session consisted of a 30-minute educational component and a 1-hour active session focusing on proper warm-up, cardio and resistance exercise, cool down and flexibility. During the summer months, the Y Kids Academy was also offered in a 1-week summer day camp format with the same eight 1.5 hour sessions integrated within 30 hours of camp activities in 4 days (Tuesday-Friday). For each YMCA location, there was one full time staff member leading the Y Kids Academy for the community and camp program formats. Each staff member was trained and supervised by the Y Kids Academy Senior Coordinator to deliver the same core curriculum, however, staff could modify the program based on the participant’s needs at each location.
Participants
The Y Kids Academy was intended for children in grade 6 and those who would be in grade 6 at the end of the summer. For the community format of the program, participants’ ages were consistent with the intent of targeting grade 6 students. However, the summer camp format of the program allowed a wider age range (9-14) so that all campers could join. All children who enrolled in a Y Kids Academy program were eligible to participate in the evaluation study.
Study information packages were distributed to the parents of Y Kids Academy participants by the research coordinator. The study information packages included a letter explaining the study, a copy of the written study consent form, and a form to indicate whether the child would require restriction from any type of PA. For the community format, study information packages were made available to families as soon as the child was enrolled, with baseline testing completed one week prior to the start of the program. For the summer camp format, families were given study information packages when they arrived on the first day of camp. Before participation in the program, baseline assessments were completed at the beginning of the second camp day if parent consent was obtained.
Parents/guardians were required to provide written informed consent for their children to participate in the evaluation activities. After written parental consent was obtained, and if the parent indicated that the child could participate in the study activities without restriction, the researcher obtained the child’s verbal assent to participate. Youth were excluded from the evaluation if they did not agree to participate, if written parental consent to participation was not provided or if children required restriction from 1 or more of the evaluation activities.
Y Kids Student Questionnaire
The Y Kids Student Questionnaire was developed specifically to evaluate participants’ knowledge about how to lead a healthy lifestyle (Appendix 1). Initially, the research team qualitatively analyzed the Y Kids Academy curriculum in order to identify major educational goals and themes. The identified priority content was then reviewed and approved by experts in youth PA and healthy lifestyles. Multiple choice questions were then sourced from published instruments to reflect the identified themes related to PA and healthy life-styles among Canadian adolescents. The draft questionnaire was circulated to managers and instructors of the Y Kids Academy and experts in youth development and healthy living for the YMCA-YWCA of the National Capital Region, who verified that the content was appropriate to the program goals. The draft questionnaire was then given to 10 youth in the target age range to verify comprehension and appropriate terminology. Responses provided by research study participants on the Y Kids Student Questionnaire were scored with 1 point for a correct answer and zero for each incorrect answer. The points awarded for all 20 questions were added together to create a total score. There were also 5 additional open-ended questions, designed to gather feedback on the Y Kids Academy program, that were not included in the quantitative evaluation of knowledge.
Y Kids Parent Questionnaire
The Y Kids Parent Questionnaire (Appendix 2), enabled parents to convey their perceptions of their children’s PA and healthy living behaviours and describe the healthy living practices within the family. The Y Kids Parent Questionnaire was completed both before and after Y Kids Academy participation. The Y Kids Academy Parent Questionnaire was composed of multiple questions addressing six topics: A) foods available to the child at home, B) the child’s physical activity, C) places for the child to be active, D) family physical activity with the child, E) the child’s use of active transportation, and F) the child’s well-being. This questionnaire was compiled from published questionnaires previously validated for use with adolescents [18-21]. When parents were asked to complete the survey a second time, they were also given an opportunity to provide open-ended feedback and comments about the Y Kids Academy and their child’s experience in the program.
CAPL Assessment
During the pre-Academy assessment, children completed the Canadian Assessment of Physical Literacy (CAPL) [22]. The CAPL assessed 4 domains of physical literacy: (1) motivation and confidence for PA, (2) knowledge and understanding of PA, (3) physical competence to perform PA, and (4) daily behaviour as evidence of engagement in a physically active lifestyle [23]. Motivation, confidence, and knowledge for engaging in PA, as well as involvement in sedentary activities was evaluated using the CAPL Knowledge of Physical Activity Questionnaire [24]. Physical competence was assessed by body measurements (BMI calculated from height and weight; abdominal fat distribution as indicated by waist circumference) and 5 different exercises. Three musculoskeletal exercises assessed grip strength, core strength (timed isometric plank hold), and flexibility (sit and reach test) [22]. The Canadian Agility and Movement Skill Assessment evaluated fundamental and complex movement skills [25]. The Progressive Aerobic Cardiovascular Endurance Run (PACER) assessed endurance. It required children to run 15 meters after each beep, with the beeps gradually increasing in frequency [26]. Finally, daily PA behaviour was measured by a pedometer worn by the children for one week. (www.capl-ecsfp.ca).
Statistical Analyses
Results from the Canadian Assessment of Physical Literacy (CAPL) were compared to scores contained in a database of CAPL results for over 3000 Canadian children using independent t-tests. Chi-square analyses compared the proportions of children in the beginning, progressing, achieving and excelling categories of physical literacy (as determined by the CAPL) among Y Kids Academy participants and the Canadian database of results. Pearson correlation examined the association between the Y Kids Academy and CAPL evaluations.
For the Y Kids Student Questionnaire, change in total score after Y Kids participation was evaluated via paired t-test between baseline and post-Y Kids scores. A secondary analysis compared the 20 answers at baseline to the answers provided at the end of the program to provide more specific information on the knowledge content areas that changed as a result of Academy participation. To adjust for multiple comparisons within these secondary analyses, a Bonferroni correction was applied (significant changes were defined as p < 0.05/20 or 0.0025). Univariate analyses initially evaluated the relationship between participant characteristics (e.g., age, gender, location, Y Kids format, pre-scores) and the change in knowledge from pre- to post-Academy (difference score). The participant characteristics that were significant or trending towards significance (p<0.10) were then entered into a multi-variable model, with backwards selection used to determine the characteristics significantly related to the pre-post difference score.
For the Y Kids Parent Questionnaire, unpaired t-tests compared pre- and post-academy scores from one group of parents whose children were enrolled in the program and from another group of parents whose children had completed the program. This analytic approach was required because most parents either did the pre-assessment (n=133) or post-assessment (n=63), with only a small proportion completing both assessments (n=40). Although pre- and post- groups were not completely independent, the unpaired t-test was the more favorable analysis since parents who repeated the assessment would be expected to have more similar scores than independent participants. A sensitivity analysis using only the paired questionnaire responses confirmed that there was no change in parent-reported scores from pre- to post-Academy (mean pre=143±16; mean post=141±26; p=0.70). All analyses were performed using the statistical software package SPSS 21 for Windows (IBM Inc., Armonk, NY, USA).
RESULTS
Study Participants
A total of 805 children were registered in the Y Kids Academy across the four participating YMCA-YWCA locations. There were 163 children who consented to the Y Kids Academy evaluation (73 female, 45%), for a study recruitment rate of 20%. Evaluation study participants ranged in age from 9 to 14 years (mean 11.1 ± 0.8), because the Y Kids Academy summer camp allowed children to participate across a broader age range. There were 81 children who participated in the 1-month community format of the program and 82 children who participated in the 1-week camp format of the program. Y Kids Academy staff recorded attendance at each session as participants required 80% attendance to qualify for the free membership upon successful completion of the program. Parent participation was higher for the pre-Academy assessment (n=133) than the post-Academy assessment (n=63).
Physical Literacy of Y Kids Academy Participants
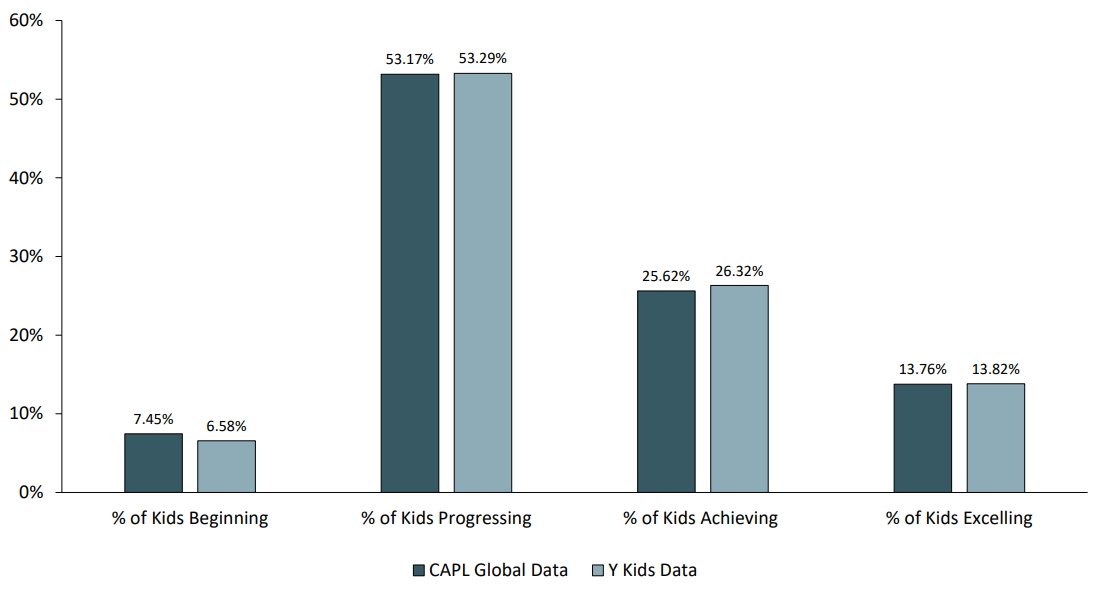
The mean total CAPL score of the Y Kids Academy participants was 62.4 ± 11.8 points. This was not significantly different (p=.071) from the mean total CAPL score (60.7 ± 11.8) we had previously measured among 3000 Canadian children (unpublished data). Among our study participants, neither age (p = 0.96) nor gender (p=0.69) were associated with CAPL score. The proportion of Y Kids Academy participants and Canadian children within each of the four CAPL interpretation categories, as shown in Figure 1, did not differ (Chi-square = 0.12, p= 0.99). The largest proportion of Y Kids Academy participants, as well as CAPL global data, were categorized as progressing at 53.29% and 53.17% respectively.
Association Between Physical Literacy and Y Kids Academy Knowledge
Knowledge scores for the Y Kids Academy evaluation were significantly associated with the physical literacy knowledge and understanding domain score at baseline (r = 0.40, p < 0.001), but not after completion of the Y Kids Academy (r = -0.16, p = 0.11). Y Kids Academy knowledge scores were not associated with other physical literacy domain or total scores at either time point (p > 0.27). The total and domain scores from the CAPL were then categorized as either “meeting” (scores rated as “Achieving” or “Excelling”) or “below” (scores rated as “Beginning” or “Progressing”) the recommended level for optimal health. Youth who “meet” the recommended level of physical literacy knowledge had significantly higher Y Kids Academy knowledge scores at baseline (mean difference ± SE: 2.1 ± 0.5 points, p < 0.001) compared to youth who were below the recommended level of physical literacy knowledge. Y Kids Academy knowledge scores at baseline did not differ between youth who did and did not achieve the recommended levels of physical literacy motivation, physical competence, daily behaviour or total physical literacy (p > 0.49). Post Y Kids Academy knowledge scores were not significantly associated with any physical literacy domains or total score. The change in Y Kids Academy knowledge score (post-baseline) was significantly smaller for participants who achieved the recommended level of physical literacy knowledge (mean difference ± SE: 2.9 ± 1.2 points, p = 0.02). Other measures of physical literacy were not associated with the change in Y Kids Academy knowledge score (p > 0.35).
Impact on Healthy Living Knowledge
Y Kids Academy Student Questionnaire responses were available for 154 participants prior to attend the course and 144 participants after attending the course. Total mean scores for the Y Kids Academy Student Questionnaire increased significantly (p<0.001) after participation in the program, with an additional 2 to 3 correct responses per child. The mean total score increased from 10.4 ± 5.4 points (out of maximum score of 20 points) at baseline to 12.7 ± 6.5 points after the program.
Change in knowledge (difference scores) was assessed for participants who did both pre- and post- Academy assessments (Table 2; n=88). In univariate analyses, change in knowledge was not associated with gender (r = 0.16; p = 0.18) or age (r = -0.13, p = 0.27). Knowledge score at baseline was significantly (r = -0.74; p<0.001) associated with the change in knowledge difference score, with a larger change occurring among those who had a lower pre-score. There were also marginal associations between difference score and program format (youth attending camp format lower; r = 0.19; p=0.08), and program location (Timothy and Russel lower than Camble; r = 0.28; p = 0.08). Based on results from the univariate analyses, participant characteristics of program format, program location, and pre-score were used to build the multi-variable model describing differences in knowledge from baseline to post-Y Kids Academy. After testing for potential interactions, there was a significant interaction (p = 0.04) between pre-score and location in relation to the Y Kids Student Questionnaire difference score. When retaining that interaction in the model, camp was not significantly associated with difference score. Therefore, the final multi-variable model was pre-score, location and the interaction between those variables (see Table 2). The model explained 57% of the variance in difference score, with a large effect size (σ2 =0.61). Pre-scores had a larger influence on the difference score at the Timothy location compared to the Russel location (p = 0.01), with no difference between other locations.
The Y Kids Student Questionnaire included 5 open ended questions that were informally summarized to identify common themes. Responses were reviewed and the number of similar responses was tabulated for each question. Participant responses described healthy lifestyles in terms of healthy eating and PA. They also described goal setting in relation to healthy lifestyles to be important for contributing to health and having something to work towards. Participants reported that the Y Kids Academy influenced their decisions about healthy eating at home, and to be more active at school and with their friends. Almost all Y Kids Academy participants (92%) said that they would recommend the program to their friends. Those who would not recommend it primarily said that their friends were already active or it was not required for their friends.
Change of Parent Perceptions
The number of parent surveys completed was 133 pre- Academy and 63 post-Academy. Approximately 1/3 of the parents who did the pre-assessment (n = 40) also did the post-assessment. There was no difference (p=0.41) in total score for the parent questionnaire when comparing the pre- and post-Academy assessments. Analyses done by each topic/section (A-F) of the parent questionnaire also found no differences in pre- and post-Academy assessments (Table 3). However, there was a strong trend (p=.07) towards parents reporting higher PA after Y Kids participation.
In the open-ended section during the post-Academy assessment, parents reported that their children had a positive experience attending the Y Kids Academy. They noted a variety of positive changes in their child’s behaviour, including being more active, making healthier food choices and drinking more water. Parents also recognized that their own behaviour had changed after the child’s participation in the Y Kids Academy. Being more active and trying to provide healthier food choices at home were commonly mentioned even though the quantitative assessments of these topics did not change. Most parents (73%) reported that the Y Kids Academy had spurred more discussions in their house about healthy lifestyles. Lastly, most parents felt that no changes were required to improve the Y Kids Academy. Those who made suggestions for improvement identified making the program longer (more weeks to complete), available to more children (grades 4 to 6), including more physically active time and having a follow up program to check in on the children’s progress and maintenance of behaviour change.
DISCUSSION
The Y Kids Academy successfully achieved its primary objective of attracting youth with both higher and lower levels of physical literacy, as evidenced by the similar CAPL scores (means and ranges) of participants compared to data from Canadian children of the same age and gender. These results suggest that the Y Kids Academy was successful in attracting a wide range of participants, including those who are among the majority of Canadian youth who do not meet current PA guidelines or have lower levels of physical literacy.
The CAPL knowledge and understanding assessment was developed to reflect Canadian physical and health education curricula [24]. The significant association between scores on this standardized assessment and baseline results from the Y Kids Academy Student Questionnaire support the validity of this new evaluation tool. Changes in knowledge with Y Kids Academy participation were significantly larger among youth whose initial levels of knowledge were lower, indicating that the program effectively targets those youth with the greatest need for enhanced knowledge about healthy living. After completing the Y Kids Academy, knowledge scores did not differ based on physical literacy knowledge, suggesting that the Y Kids Academy curriculum enabled youth with low levels of healthy living knowledge to improve their knowledge to a level comparable to their peers.
Children’s knowledge of healthy living total score improved significantly after participation in the Y Kids Academy, regardless of the participants’ physical literacy, with the biggest change among those with lower knowledge scores at baseline. Responses to open-ended questions indicated that the Y Kids Academy influenced participants’ decisions about healthy eating at home and encouraged them to be more active at school and with their friends. These results suggest that the Y Kids Academy had a positive effect on participants’ knowledge of how to lead a healthy lifestyle. Questionnaire responses from parents regarding the healthy living behaviours of their youth did not differ from pre to post Y Kids Academy, but parent comments indicated that attending the program resulted in positive changes to both the youths’ and parents’ behaviors, as well as increased discussions in their households about healthy lifestyles.
Y Kids Academy knowledge scores tended to differ by program location at baseline. There was also a significant interaction between program location and baseline knowledge score in relation to the magnitude of change in knowledge with Y Kids Academy participation. Although not measured in this study, anecdotal evidence suggests that there may be socio-economic differences between the communities adjacent to each YMCA location in this study. The Timothy location was in the heart of downtown, Ranger and Camble locations were in suburban areas, and Russel was in a smaller rural area outside of the city. Participants from downtown and rural areas had lower levels of healthy living knowledge at baseline as well as a greater gain in knowledge after participation in the program, compared to participants from suburban areas. Further research is required to investigate the potential impact of socio-economic variables on healthy living knowledge and the benefits of the Y Kids Academy program.
Recent research has suggested that health-related fitness knowledge can predict PA behaviour and physical fitness [27]. Ferkel et al. [27] suggests that having appropriate PA knowledge may be critical for understanding and applying exercise principles to daily life. Although research in the area is limited, education interventions have been shown to result in a longitudinal increase in PA and fitness. However, if an individual does not possess adequate knowledge related to the importance of exercise and how to structure a PA or fitness program, he or she may be more likely to discontinue PA as adults [28]. As such, the knowledge participants gain from educational PA interventions, such as the Y Kids Academy, may enable them to maintain training more effectively over time. Therefore, future studies should investigate the longer term impact of the increase in healthy living knowledge from Y Kids Academy participation on subsequent healthy living behaviour.
The Y Kids Academy was successful at attracting participants who have lower levels of physical literacy. A majority (60%) of the participants were beginning or progressing on their physical literacy journey. This is important because it demonstrates that the Y Kids Academy was able to attract the young adolescents most in need of this type of intervention. This differs from the reports of most PA intervention studies, because research participants must volunteer to complete the study, and typically these individuals are already motivated to do exercise [28]. This bias towards more active study participants has been clearly described in the findings of a 2016 review [29] of PA interventions for youth. Mears and colleagues found that none of the identified studies in their review demonstrated that participants who consented and participated in the trials were similar in baseline demographics and activity levels to those who did not. As such, a significant strength of the present study is inclusion of the CAPL results at baseline, which demonstrated that study participants were representative of the population of Canadian children.
PA declines during adolescence [11], and longitudinal studies have suggested that this reflects a decline in organized sport participation [30,31]. Proposed explanations for sport dropout during adolescence include difficulty balancing school, work, and friends with sport, as well as increased pressure to attend social gatherings [32]. A lack of confidence, including ‘not being good enough’ and ‘not being as good as I wanted to be’ [32] or feeling embarrassed to ‘fail’ in front of their peers are also recognized as important contributors to sport dropout during adolescence. The Y Kids Academy was designed with a focus on preparing pre-adolescents to perform PA using standard conditioning equipment. It was hypothesized that the increased independence of personal exercise programs would offer a more flexible time commitment than organized sports, which theoretically would allow adolescents to remain active while balancing other aspects of life. It was also believed that pre-adolescents would be attracted to the opportunity to use the conditioning facilities that were normally reserved for older adolescents and adults. In addition, the ability to perform exercise on one’s own may be a more appealing to adolescents who lack the self-confidence to engage in PA in front of their peers.
The comments and feedback from both youth and their parents indicated very high levels of support for the Y Kids Academy. Almost all participants (92%) said that they would recommend the program to their friends, unless they were already active. Most parents felt that no changes were required for the program. However, parents who did make suggestions wanted to make the program longer, have it available to a wider age range, include more physically active time, and have follow up to monitor longer-term progress and maintenance of behaviour change.
The main limitation of this study is that the evaluation of the Y Kids Academy Program did not include a control group. As such, the improvement in knowledge scores from pre- to post-assessments cannot be attributed to increased knowledge of participants. Moreover, it is not clear whether these changes would be sustained over the long term and if these changes in knowledge would lead to changes in physical literacy or healthy living behaviour over the longer term. Studies that directly measure the physical literacy and healthy living behaviours of Y Kids Academy participants over a longer period of time are required in order to evaluate the long-term impact of Y Kids Academy participation. Recommendations to include a control group, increase the length of the program or provide a subsequent follow up program may further enhance the impact of the program and our ability to measure whether those impacts are sustained.
The Y Kids Student Questionnaire was developed specifically for this project. Validity of the questionnaire was assessed through expert review by those who created the Y Kids Academy program and comprehension of item wording was verified through pilot testing. The relationship between Y Kids Student Questionnaire scores and a standardized assessment of physical literacy knowledge also support the validity of this new instrument. However, test-retest reliability assessments are recommended to strengthen the psychometric properties of the Y Kids Student Questionnaire.
CONCLUSIONS
This initial evaluation of the Y Kids Academy indicated that it effectively attracts participants representative of Canadian youth, of whom 60% were not yet achieving the recommended level of physical literacy. Furthermore, larger changes in knowledge among youth with lower initial knowledge scores suggests that the Y Kids Academy content effectively targets youth with the greatest need for changes to their healthy living knowledge. Lastly, this pilot evaluation of participants’ pre- and post-Y Kids Academy knowledge scores suggests that the program may have potential for improving knowledge related to a healthy, active lifestyle among young adolescents.