Bag Carrying Method during Level Walking Affects Perceived Exertion Ratings without Altering Energy Cost, Oxygen Consumption, and Heart Rate in Healthy Adults: A Randomized Crossover Trial
Article information

Abstract
OBJECTIVES
Little is known regarding the associations between Borg’s rating of perceived exertion (RPE), cardiopulmonary responses, and carrying bags while level walking. We investigated the changes in RPE and cardiopulmonary responses, including energy cost (EC), oxygen consumption (VdotO₂), and heart rate (HR), when walking with a bag.
METHODS
This randomized crossover study included 10 healthy adults (aged 21–22 years). Four days of experiments were performed at intervals of 1–2 weeks. The participants walked on a level treadmill while carrying a bag with a strap weighting 5 kg, placed diagonally on their shoulders (DS), vertically on their shoulders (VS), vertically in one hand (VH), and on their backs using both shoulders (BS) for 20 min. Walking speed was stable among all experiments, and was set to the participants’ preferred speed.
RESULTS
No significant differences between bag carrying methods regarding EC, VdotO₂, and %HRreserve (based on HR) were observed, whereas RPE respiratory (RPE-resp) and RPE leg muscle (RPE-leg) scores varied based on bag carrying method used. RPE-resp score was significantly lower for DS and BS than VH (both p < 0.0083); however, no significant difference was observed when each RPE-leg score was compared.
CONCLUSIONS
We found that RPE-resp score varied, whereas no changes in EC, VdotO₂, and HR were observed in healthy adults while walking with different bag carrying methods. Additionally, of all bag carrying methods assessed, the highest RPE-resp score was observed when individuals carried a bag with one-hand at their side.
INTRODUCTION
People often walk with bags of various sizes, since the carrying of luggage for work, travel, and shopping is common. Bags come in various styles, and one-handed, two-handed, one-shoulder, or two-shoulder (a backpack) carrying methods are used based on individual preference and situation (e.g., commuting), weight, and shape of luggage.
Although walking with a bag is useful for carrying luggage, it sometimes has an adverse effect on the body and may increase risk of lower back pain and strain on fingers, wrists, and shoulders [1,2]. Additionally, differences in bag carrying methods may influence walking performance (e.g., gait posture, walking cadence, and muscle activity) [1-3]. Furthermore, carrying a load in a single bag against body chest might increase heart rate (HR) more than it would if a bag was held using both sides of the body to distribute the weight, due to differences in balancing the load carried [1].
To the best of our knowledge, limited research has been performed that has quantified cardiopulmonary response differences based on bag carrying method. Further, the association between the bag carrying method and perceived exercise intensity, such as Borg’s rating of perceived exertion (RPE) scale [4], which is strongly correlated with HR [5], remains unknown. Therefore, we hypothesized that cardiopulmonary response and RPE during walking might differ based on bag carrying method, especially when loads are carried on one side of the body due to weight imbalance. Individuals may benefit from choosing a method that best suits their purpose, such as conserving energy, minimizing psychological stress, or conversely, increasing energy consumption. In this study, we investigated changes in RPE and cardiopulmonary response in healthy adults, including energy cost (EC), oxygen consumption (VdotO₂), and HR, when walking using four bag carrying methods.
METHODS
Study Participants
Twelve healthy adults (aged 21–22 years) who attended a single university and volunteered for this study from April to August 2019 were enrolled in the study. Enrolment was not based on their typical bag carrying preference, since we believed that it would not influence the results of the study. Participants with motor dysfunction (e.g., knee osteoarthritis), other diseases affecting physical activity (PA), a body mass index, ≥ 25 kg/m2 (overweight/obesity), and high volumes of usual PA (at least 150 minutes of moderate-intensity PA or at least 75 minutes of vigorous-intensity PA per week) [6] were excluded. No participants took medications, nor did they receive medical, nutritional, or physical education for the management of metabolic functioning before or during the study. Written informed consent was obtained from all participants. The institutional review board of Aino University (Ibaraki, Japan) approved the study protocol (approval number: 2019-04) in accordance with the Declaration of Helsinki.
Experimental Design
This was a randomized crossover study. We set a schedule for performing four walking experiments, which were separated by 1–2-week periods (Figure 1). We asked participants to consume meals and perform activities of daily living and regular exercise (if any) as usual. The type of meal consumed before and during experimental testing was not specified. One day prior to the experimental evaluation, participants had dinner in their homes before 9 p.m., and on the day of experiments, they had breakfast in their homes between 7 and 8 a.m. and lunch at the university between 12 and 1 p.m. We instructed participants to refrain from consuming additional foods, drinks containing caffeine and alcohol, and smoking on the day before and on days they were evaluated.

Study flow chart
Exercise protocol
More than four hours after lunch, participants were asked to walk on a level treadmill (Auto Runner AR-200, Minato Medical Science Co., Ltd.; Osaka, Japan) while carrying a bag and wearing their usual shoes. The treadmill walking program included a 20-min exercise period, which was used to assess different bag carrying methods. Prior to exercise, there was a 3-min warm-up period, and exercise was followed by a cool-down. Bag carrying methods assessed were as follows: 1) diagonally on a shoulder (DS), 2) vertically on a shoulder (VS), 3) vertically in one hand (VH), and 4) on the back using both shoulders (BS) (Figure 2). The main material of all bags was nylon, and the weight load was set at 5 kg, including the bag weight, which was based on a preliminary survey that assessed the weight of the participants’ usual luggage (e.g., textbook). Participants walked at their preferred speeds (Table 1), which were evaluated without carrying any bags before the experiments were initiated. The speed during the warm-up and exercise periods were stable among the experiments, whereas participants could freely adjust the cool-down treadmill speed.
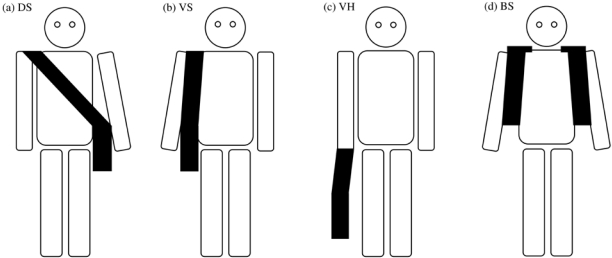
Bag carrying methods assessed
(a) DS (carrying diagonally on a shoulder): placing bag body at the level of the greater trochanter on the dominant hand side; (b) VS (carrying vertically on a shoulder): placing bag body at the level of the greater trochanter on the non-dominant hand side; (c) VH (carrying vertically in one hand): grasping the bag belt (20 cm in length) with the dominant hand; (d) BS (carrying on the back using both shoulders): placing the top edge of bag body at the level of the inferior angle of the scapula.

Characteristics of the study participants
Measurements
Measurements monitored during the exercise period were as follows: EC, VdotO₂, HR (%HRreserve), and respiratory and leg muscle Borg 6–20 RPE scale [4] (RPE-resp and RPE-leg, respectively). EC and VdotO₂ were monitored using respiratory gas analysis (Aero Monitor AE-300S, Minato Medical Science Co., Ltd.; Osaka, Japan). HR was recorded using a Polar Accurex Plus monitor (Polar Electro; Kempele, Finland). Resting HR (the lowest HR measured while each participant laid for 15 min in a supine position) and mean HR during the exercise period were measured, and using these values and HRmax (220 - age), %HRreserve was calculated as follows: (mean HR - resting HR) / (HRmax - resting HR) × 100 [7]. RPE scores were recorded immediately after the exercise period. The room temperature during the experiments maintained between 23°C and 25°C.
Statistical Analysis
All continuous variables were reported as means and 95% confidence interval (CI), and ordinal variables were reported as medians and 95% CI. The bag carrying method variables were compared using one-way repeated measures analysis of variance (ANOVA) or the Friedman test, followed by the post hoc Wilcoxon signed-rank test with a Bonferroni correction, using IBM SPSS statistics software (version 20.0, IBM; Tokyo, Japan). Statistical significance was set at p < 0.05 for ANOVA and the Friedman test, and at p < 0.0083 (the p-value was calculated as follows: 0.05/number of tests; 0.05/6) for the post hoc test. Additionally, post hoc effect size (r = Z/√n) calculation was performed for each variable, using G*Power (version 3.1.9.4., Heinrich-Heine University; Düsseldorf, Germany).
RESULTS
After the experiments, two participants were excluded from the analysis due to the absence of data, and the data of 10 participants were analyzed (Figure 1). Characteristics of participants included in the final analysis are shown in Table 1. Additionally, VdotO₂ and HR data measured during exercise are shown in Figure 3.

Time-course changes in VdotO2 (a) and heart rate (b)
Values are presented as mean. DS: carrying diagonally on a shoulder; VS: carrying vertically on a shoulder; VH: carrying vertically in one hand; BS: carrying on the back using both shoulders.
ANOVA revealed no significant differences in EC, VdotO₂, and %HRreserve (p = 0.49, p = 0.12, p = 0.56, respectively) based on bag carrying methods, whereas the Friedman test showed that RPE-resp and RPE-leg scores differed (p < 0.01, p < 0.05, respectively) (Table 2). Post hoc analysis showed that bags carried using DS and BS produced RPE-resp scores that were significantly lower than those of VH (p = 0.005, r = 0.90; p = 0.004, r = 0.90, respectively); however, no significant differences were observed when RPE-leg scores were compared.
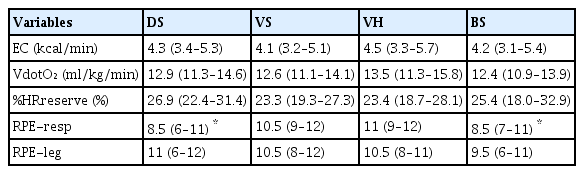
Comparison of outcomes among bag carrying methods
DISCUSSION
We found that RPE-resp score changed depending on the bag carrying methods, and of all bag carrying methods considered, the VH method produced the greatest score in healthy adults. Moreover, this difference was not accompanied by any changes in EC, VdotO₂, %HRreserve, and RPE-leg score. To the best of our knowledge, this is the first study to reveal these results.
RPE-resp significantly increased when walking with a bag using the VH method, compared to DS and BS. One-hand carrying while walking may induce psychological stress (e.g., fatigue and respiratory distress) as well as the changes in gait posture and muscle activity, compared to the other methods, which involve carrying the bag on the shoulder(s) and back, due to imbalance while walking [3,8]. Thus, RPE-resp score, which subjectively measures psychological strain during exercise [4], might differ depending on the type of bag carrying method employed in this study. Additionally, a change in RPE-resp score was observed without accompanying changes in other parameters. RPE score predicts oxygen uptake and HR [5,9]. However, RPE-resp score may not correlate with cardiac response, especially within the 20-min that follows the initiation of low-intensity exercise [10]. Conversely, it has been suggested that RPE-leg score may correlate with HR, regardless of exercise intensity [10]. Therefore, RPE-resp score associated with carrying a bag in one hand while walking might increase without any changes in cardiac and metabolic responses and RPE-leg score, due to the low exercise load assessed in this study (20%–30 %HRreserve).
Previous studies have shown that physiological response, including cardiac response, while walking differed based on bag carrying method. It was previously shown that two-handed bag carrying was associated with a lower HR, percent muscle activity of maximum voluntary contraction (%MVC) in the hand, forearm, upper arm, and shoulder muscles, and subjective discomfort rating, assessed locally perceived discomfort method, than did one-handed bag carrying [11]. Additionally, a previous study indicated that cardiovascular stress, including HR, was 10% greater when a single bag was carried at the chest than that when held at the sides of the body [1]. Furthermore, carrying a double-strap bag (golf bag) might require less VdotO2 and require a lower HR than a single-strap bag [12]. In this study, cardiac responses did not vary based on bag carrying method, even for one-handed bag carrying (VH). This may have been a result of low degree of load imbalance produced in the study. The load of bag in this study was 5 kg, which was lower than that of a previous report that assessed effects of carrying the following loads [11]: 50, 100, and 150 N (approximately 5, 10, and 15 kg, respectively). The study showed that there were significant differences in cardiac cost observed based on the bag carrying method employed when effects of carrying a 100 N and 150 N load were assessed, but no difference was observed when a 50 N load was examined. Thus, the load in this study likely did not influence physiological responses. Moreover, walking speed, which in the present study was lower than reported speeds of individuals under 30 years of age (median value: 4.8 km/h [13]), might have affected metabolic response findings, including EC. Further, whether the bag was carried on the upper or lower back also could potentially affect EC [14]. Therefore, further research that involves a more rapid walking speed and assesses additional bag carrying methods (e.g., backpack on the upper/lower back) is needed to further investigate whether there is an association between cardiac and metabolic responses and bag carrying while walking.
A strength of this study is its unique nature. To our knowledge, no previous study has investigated the association between bag carrying bag method, cardiac and metabolic responses, and RPE scores. We believe that our findings will contribute to the management of metabolic outcomes and the reduction of psychological stress while walking. However, there are some limitations to this study. First, this was a single-center study with a small sample size, which recruited healthy, young, and sedentary participants. Second, as indicated previously, the walking speed used in this study was relatively slow; hence, research involving several walking speeds may be needed. Third, the results of this study may have been affected by the volume and content of the most recent meals consumed by participants. Food intake may have affected energy expenditure over an 8-h period [15]. Fourth, the kinematic parameters, such as gait posture (e.g., round back), muscle activity (e.g., %MVC), and walking stability (e.g., center of gravity sway) were not measured. Therefore, further studies, which involve a greater number of participants and assess other types of populations like the elderly, are needed to confirm the clinical relevance of selecting a proper bag carrying method when walking.
CONCLUSIONS
In summary, we found that RPE-resp score varied based on bag carrying method without any changes in EC, VdotO₂, and HR in healthy adults while walking. Additionally, of the four bag carrying methods assessed, the highest average RPE-resp score was observed when participants employed the one-handed at one side carrying method. Although further studies are needed, we propose that it may be important to consider these characteristics when managing individuals’ psychological stress and cardiac and metabolic characteristics while walking.
Acknowledgements
The authors thank the study participants for their time and effort.
Notes
Conflict of Interest
The authors declare no conflict of interest.