
INTRODUCTION
Sports injuries are defined as any kind of damage to body tissues caused by a large external force applied during sports activities, while sports disorders are defined as minute damage to body tissues caused by repeated application of a causative action (load). It is believed that physical factors (internal factors), environmental factors (external factors), and training factors (triggering factors) related to the quantity and quality of the causative action are involved in the development of sports injuries. Some internal factors are difficult to modify (i.e., age, gender, and anatomical characteristics), but there are also others that are modifiable through training (i.e., muscle strength, muscle tightness, and dynamic alignment) [1,2]. Sports activities place a greater load on body parts than daily life, and these can occur in any part of the body, including the head, neck, limbs, trunk, and internal organs. Therefore, we believe that it is important to modify internal factors and how to prevent and minimize sports-related injuries.
Preventive approaches to reducing sports injuries are important. First, the problem needs to be identified and described in terms of the incidence and severity of sports injuries. Second, the factors and mechanisms involved in the occurrence of sports injuries are identified. Third, countermeasures that can potentially reduce future risks are introduced. These measures should be based on the etiology and mechanisms identified in the second step. Finally, the effectiveness of the countermeasure must be assessed [3].
Many people perform warm-up (W-up) before exercise to prevent trauma and injury, as well as to improve performance. The main purpose of W-up is to increase body temperature [4,5], which causes an increase in oxygen dissociation from hemoglobin and myoglobin, an acceleration of metabolic reaction rate, nerve conduction velocity and nerve transmission, increased in blood flow in active muscles, and increased oxygen uptake. All these physiological factors contribute to improved performance [4,5].
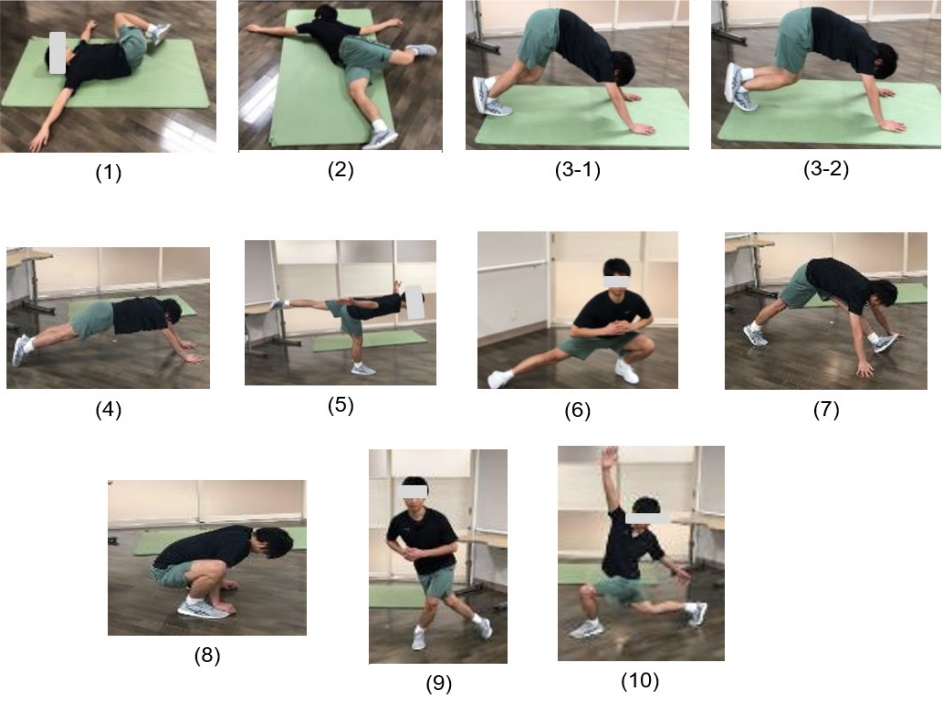
Core training is one of the most important training methods for improving performance and preventing sports injuries. The core is the center of the body and consists of the scapula, rib cage, abdomen, lower back, pelvis, and hip joints, excluding the limbs. Verstegen [6,7] states that in order for the core to function, it is necessary to have perfect posture, which minimizes stress from external forces and allows the major joints to work most efficiently against gravity. On the other hand, performance in an unstable posture puts stress on the body and increases the possibility of movement-related injuries. Training to improve the function of the core includes movement preparation (MP), which aims to improve joint mobility and muscle flexibility in preparation for physical activity. MP involves repeated stretching and contraction of muscles in response to joint movement, which increases core muscle temperature. MP is effective when performed as a W-up because it increases the temperature of the trunk muscles by repeatedly stretching and contracting the muscles as the joints move.
Because of its benefits in increasing the muscle temperature of the trunk and improving flexibility, MP is also expected to be effective as a W-up. However, only a few reports discuss the effectiveness of MP as a W-up in preventing trauma and injury. The purpose of this study was to clarify the effect of MP on the prevention of injury in male high school soccer players. The period of conventional W-up was used as the control period, while the period with MP was used as the intervention period (IP).
METHODS
Study Participants
The study subjects were 55 first-year to third-year members of a high school boys' soccer team (age: 15.9 ± 1.0 years, height: 168.5 ± 5.2 cm, weight: 57.4 ± 5.3 kg). Those with orthopedic diseases at the time of measurement and those who did not participate in practices or games were excluded. We also excluded subjects who had difficulty in measurement or who withdrew their consent.
Ethical Considerations
This study was conducted in the spirit of the Declaration of Helsinki and in compliance with the Ethical Guidelines for Medical Research Involving Human Subjects of the Ministry of Health, Labor and Welfare and the Ministry of Education, Culture, Sports, Science and Technology, in order to protect the human rights, maintain the safety, and improve the welfare of the research collaborators, as well as to ensure the scientific quality of this study and the reliability of the results. This research was conducted after sufficient written and oral explanations were given to the research collaborators, their guardians, and school principals, and after consent was obtained. The study was approved by the Ethics Committee of Takasaki University of Health and Welfare (Takasaki Health University Ethics No. 3081).
Research Flow
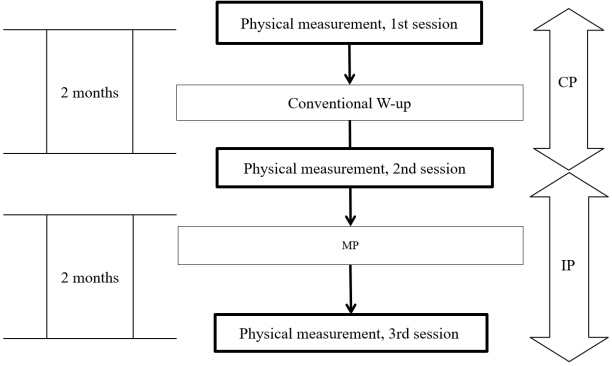
The measurement of items such as flexibility, balance, and performance were collectively referred to as physical measurements. Physical measurements were performed three times, with an interval of two months between the dates of the measurements. The first physical measurement was conducted before testing. The following two months, respectively, were designated as the CP, wherein the team conducted the conventional W-up program, and the IP, wherein the team conducted the MP with the W-up program (Figure 1). The W-up program during the CP included running, static stretching, then dynamic stretching. On the other hand, the W-up program during the IP included running then MP.
Inspection and Measurement Items
a. Basic Information
All subjects were given a form to fill in their height (cm), weight (kg), kicking foot, and axle foot; each athlete filled in the form individually. The kicking leg was defined as the leg that was frequently used for shooting and passing during play and was primarily used to control the ball, whereas the opposite leg defined the axle leg.
b. Flexibility
Flexibility of the posterior thigh (°)
To measure the flexibility of the posterior surface of the thigh, the angle of straight leg raising (SLR) was measured, and the angle between the thigh and the floor surface was measured in 1° increments at the position where light resistance was felt.
c. Flexibility of trunk and lower limbs (cm)
The finger floor distance (FFD) was measured as a method to measure the flexibility of the body. The measurement was performed using a digital forward flexion meter (Takei Equipment Co., Ltd., Friction-D). The distance between the tip of the middle finger and the floor of the table was measured in 0.1 cm increments.
d. Flexibility of the front of the thigh (cm)
The heel-buttock distance (HBD) was assessed as a measure of the flexibility of the anterior surface of the thigh. The distance between the heel and the front of the thigh was measured in increments of 0.5 cm by pushing the distal lower leg while the knee joint on one side was flexed in a prone position.
e. Flexibility of the back of the lower leg (°)
The lower leg inclination angle was assessed as a measure of the flexibility of the posterior surface of the lower leg [8]. In the starting limb position, the measured lower leg was stepped forward and fully tilted forward toward the examinee, taking care that the heel did not leave the floor while the entire sole of the lower limb was grounded. The axis of movement was the fibula, and the angle between the fibula and the ground was measured in 1° increments, with the vertical line from the ground being 0°.
f. Dynamic Balance
The modified Star Excursion Balance Test (mSEBT) is one of the indices to evaluate dynamic balance ability in a one-legged stance, and it has been reported as a tool to predict lower limb disorders [9-12]. A sheet with increments of 1 cm on a line extending in 3 directions (anterior, posterolateral, and posteromedial) was placed on the floor[9-12]. The maximum reach distance was measured in 1 cm increments, with the tip of the toe in the one-legged stance being 0 cm, the plantar surface of the supporting leg not leaving the floor, and the weight not being placed on the apex of the reaching leg during reaching. The maximum reach distance was measured in 1 cm increments, and the mean value was divided by the length of the spinal malleolus distance.
Performance
a. Sprint time (sec)
The time of the 40-m sprint was measured using a stopwatch. The starting posture was a standing start, and the time when runners passed the 40 m mark from the start was measured. Measurements were taken twice, and the smallest value rounded off to the second decimal place was used.
b. Vertical jump height (cm)
The vertical jump height was measured using a yardstick (S&C Co., Ltd., Yardstick). From a stationary standing position, the left or right upper limb was raised, and the tip of the finger was set as the starting line. The subjects were instructed to jump vertically on the spot and touch the yardstick at the highest point, with or without arm recoil. The height from the starting line to the highest point was measured as the jumping height in 1 cm increments. The measurements were performed twice, and the maximum value was adopted.
Injury Status
Based on previous studies [13,14], an injury was defined as non-participation in practice or games for more than one day. Based on the number of occurrences of injury, we calculated the incidence of injury by time, as well as recorded the site, severity, cause, and type of injury per 1000 practice sessions (/1000 athlete-exposure [/1000 AE]).
The injury incidence rate was calculated using the following formula: total number of injuries ÷ total number of practices and games × 1000 = injury incidence rate. The incidence of injury in practice was calculated by using the following formula: number of injuries that occurred in practice ÷ total number of practices × 1000 = incidence of injury. The incidence of injury in games was calculated using the following formula: number of injuries/disabilities that occurred in games ÷ total number of games × 1000 = incidence of injury. Injuries were investigated by the principal investigator, who visited the subjects once a week and interviewed them.
Intervention Method
The W-up program during the CP started with running, static stretching, then dynamic stretching, whereas during the IP, this started with running then MP. The W-up program was set to be a total of 15 min during both time periods.
Dynamic Stretching
Each dynamic stretching movement was performed 10 times with light recoil (Figure 4).
Date Analysis
The risk ratios and 95% confidence intervals for the CP versus the IP were presented and discussed using a χ² test of independence. The number of days required to return to practice and games for each injury were compared between the CP and the IP. The normality of the return time was confirmed using the Shapiro–Wilk test, while the Mann–Whitney U test was used for comparison because normality was not found.
The Shapiro–Wilk test was performed to confirm normality for all items obtained from the first, second, and third physical measurements. Since no normal distribution was observed, the Friedman test was performed, followed by the Wilcoxon signed rank test as a subsequent test. The p-values were corrected and compared using the Bonferroni method. All data were analyzed using the Statistical Package for Social Science (SPSS, version 22). For all statistical tests, P < 0.05 was considered significant.
RESULTS
Comparison of the Incidence of Injury Between CP and IP (Table 1)
a. Injury Incidence
During the 2-month CP and IP, respectively, a total of 12 and 7 injuries/disabilities occurred, with an incidence of 3.91/1000 AE and 2.26/1000 AE, with no significant difference (P = 0.278). The number of injuries/disabilities occurring during practice was 8 for the CP and 2 for the IP, with injury incidence rates of 3.58/1000 AE and 1.28/1000 AE, respectively (P = 0.060). Furthermore, the number of injuries/disabilities that occurred during games was 4 in the CP and 5 in the IP, with injury rates of 4.80/1000AE and 3.25/1000AE, respectively (P = 0.452).
b. Severity of Injury and Return to Work Days
The incidence of injury by severity for CP and IP, respectively, were as follows: 2.61/1000 AE and 1.61/1000 AE for very mild; 0.33/1000 AE and 0.00/1000 AE for mild; 0.33/1000 AE and 0.65/1000 AE for moderate; and 0.33/1000 AE and 0.65/1000 AE for severe.
The median number of days to return to work (1st–3rd quartile) was 7.0 (range: 3.0–16.0) days for CP and 7.0 (range: 6.8–15.3) days for IP, with no significant difference (P = 0.550).
Causes of Injury and Site of Injury
The CP and IP, respectively, had incidences of 1.96/1000 AE and 1.61/1000 AE for contact injuries. The CP and IP were 1.96/1000 AE and 0.65/1000 AE for non-contact injuries. The CP and IP for the lower limbs were 1.96/1000 AE and 1.29/1000 AE, respectively.
Comparison of Changes in Physical Measurements Between the CP and IP (Table 2)
In terms of flexibility, the SLRs of the kicking leg and the axle foot showed a significant increase from the first to the third measurement (P < 0.001). Similarly, the HBD of the kicking leg (P = 0.004) and the axle leg (P = 0.009) showed a significant improvement in the second round compared to the first round.
In terms of balance, the anterior reach ratio of the kicking leg and the axle leg showed a progressive increase in reach ratio across all three measurements, and there were significant differences between the first and second times, and between the first and third times (kicking leg: P < 0.001, axle leg: P < 0.001). The kicking leg and axle leg of the posterior lateral reach rate and posterior medial reach rate decreased in the second round compared to the first round, whereas the reach rate increased in the third round compared to the second round.
In terms of performance, the vertical jump height showed progressive expansion all 3 times. The vertical jump height was larger during the second time compared to the first time, and in the third time compared to both the second and first times (1st–2nd: P = 0.011, 2nd–3rd: P < 0.001, 1st–3rd: P < 0.001). The 40-m sprint time did not differ significantly between the measurements.
DISCUSSION
Effectiveness in Preventing Injury
The incidence of injury during the IP decreased by about 42% compared to the CP. Furthermore, the incidence of injury during practice and games was reduced by about 63% and 32%, respectively. Furthermore, when comparing the causes of injury, the incidence of contact and non-contact injury was reduced by about 18% and 64%, respectively. However, since there was no statistically significant difference between the two periods in this study, it was not possible to fully confirm whether MP was effective in preventing sports injuries as a W-up.
According to a report by Bahr [1], internal factors such as muscle strength, muscle tightness, and dynamic alignment are involved in the occurrence of sports injuries caused by non-contact mechanisms. In addition, previous studies [15-17] have shown that incorporating dynamic stretching into a W-up program can improve flexibility, balance, and performance more than static stretching alone. The MP conducted in this study is also a type of dynamic stretching, and since it has been shown to improve flexibility and balance functions, which are internal factors, it is possible that the effects of trauma and disability can be confirmed upon further investigation. One of the factors that prevented us from finding statistically significant differences in this study is the possibility that the low incidence of trauma and disability may have affected the results. This study was conducted for a period of two months, but most of the previous studies that reported the occurrence of sports injuries and disabilities were conducted for over a year. Therefore, it is necessary to continue the survey and to extend the survey period to more than one year.
Results of Physical Measurements
The results of physical measurements showed that flexibility and balance were improved by the implementation of MP. After the intervention of MP, there was a tendency for improvement in the items of flexibility at the third measurement. In addition, although no significant difference was found, a significant difference was also found in the FFD item measured with a movement similar to the Smooth Squat to Stand. Furthermore, improvement was also seen in the flexibility of SLR and leg tilt angle, which measures the tightness of the hamstrings and triceps, respectively. Flexibility is considered an internal factor in the occurrence of sports injuries, thus increasing and improving flexibility may lead to a decrease in the occurrence of injuries [18-20].
The results of the mSEBT, which measures dynamic balance ability, showed a tendency to improve over the two months of intervention, with a significant improvement in the forward reach rate. In a previous study using the mSEBT [11, 21], a correlation was found between the ankle dorsiflexion angle and the forward reach rate. Similarly, we found that the ankle dorsiflexion angle correlated with the forward reach component of the mSEBT in our study. The calf-stretching performed in the W-up program of this study was intended to improve the flexibility of the posterior muscles of the lower leg, and this may have contributed to the improvement of the anterior reach rate by expanding the lower leg tilt angle. In addition, it is said that a decrease in the anterior reach rate is related to sports injuries of the ankle and knee joints [9-12]. In this study, we believe that an increase in the anterior reach rate reduced the incidence of lower limb injuries by approximately 34%.
Limitations
A limitation of this study is that all physical measurements were taken outdoors. Considering that temperature and humidity could affect the results of the measurement, it would have been ideal to have a consistent environment for measurement indoors. However, since this study was conducted during club activities, the measurements had to be taken outdoors to reduce the impact on club activities. Therefore, environmental factors may have affected the results of the physical measurements. Since the duration of this study was short, it is necessary to continue investigating the occurrence of sports injuries for long-term verification and prevention.
CONCLUSIONS
MP was used as a W-up to examine its effectiveness in preventing sports injuries and disorders and changes in physical function. There was no statistically significant difference in the number of incidents of trauma and disability between CP and IP, and we could not fully confirm the effectiveness of MP as a W-up in the prevention of sports trauma and disability. However, when comparing the percentages calculated from the number of injuries and disabilities, the incidence of injuries and disabilities was lower in IP. In particular, the incidence of trauma and disability during practice and the incidence of trauma and disability caused by non-contact types were found to be significantly reduced.
MP contributed not only to the improvement of flexibility, but also to the improvement of balance function related to flexibility. Therefore, it may be possible to prevent sports injuries by clarifying muscle stiffness, which is closely related to factors of sports injuries, and adding new MP to the W-up to improve muscle stiffness.