Changes Observed in the 6-minute Walk Test in Response to Exercise-based Cardiac Rehabilitation
Article information

Abstract
OBJECTIVES
The six-minute walk test (6MWT) is widely used in exercise based cardiac rehabilitation (EBCR) for assessment of functional capacity. The purpose of this study was to assess the effect of structured exercise in an EBCR program on 6MWT change and to determine the significance of age, gender, body mass index (BMI), pathology and exercise attendance on influencing this outcome.
METHODS
Data from a single centre 6-week (twice weekly exercise and education of one-hour duration) exercise-based cardiac rehabilitation program were analysed. Between 2006 and 2019, 2524 patients (males 1923, females 601, mean age 63.5 ± 11.2 years) with cardiovascular disease completed a pre and post 6MWT. Analysis included the effect of age, gender, pathology, BMI and exercise attendance on 6MWT outcome.
RESULTS
The group mean improvement in the 6MWT was 21.8% (pre 6MWT 432 ± 83, post 6MWT 527 ± 102 metres). The age-related improvement showed that both males and females achieved a post 6MWT results equivalent to the pre 6MWT result of patients two decades younger with improvement in the 6MWT unrelated to exercise attendance.
CONCLUSIONS
The 6MWT provides simple safe method for assessment of functional capacity in an out-of-hospital environment being suitable for all ages. The post EBCR 6MWT results showed a group mean improvement in excess of 20% for both sexes. The decline per decade in 6MWT distance is less than 20 metres up to the sixth decade with a more marked decline from the sixth to the eighth decade, the decline being approximately 40-metres for both sexes in the eighth decade.
INTRODUCTION
In medical management we depend on a multitude of tests to define pathology and assist with clinical decision making. Many of the clinical targets used in cardiovascular disease are defined by numerical values where the aim of clinical intervention is to improve outcome as shown by a change in a measured value of a test, attempting to ‘normalize’ that value or to move towards a desired target. Exercise-based cardiac rehabilitation (EBCR) is an example of a clinical intervention and cardiorespiratory fitness (CRF) an example of a clinical outcome or target. The six-minute walk test (6MWT) is the most commonly used test for assessment of CRF in EBCR. Guidelines for use of this test were formalized in a publication by the American Thoracic Society (ATS) in 2002, the perceived value being its safety for unlike a maximal exercise test, it is considered safe to be performed in a non-hospital environment [1].
The ATS recommends the use of the 6MWT for determining functional capacity, either as a single measurement that can be used for prognostic assessment for long term morbidity and mortality, or repeated measurement to assess the response to a therapeutic intervention [1]. As such, the 6MWT acts as a surrogate measure of oxygen uptake as studies have shown a moderate to high correlation with maximal (peak) oxygen uptake (VO2peak), particularly with more severe degrees of cardiovascular disease [2-8], with a simplified equation predicting VO2peak from the single variable of 6MWT distance [7]. To assess response to an intervention the use of an absolute value is recommended, e.g. an increase in walking distance of 50 metres as opposed to a percentage increase in the 6MWT distance [1] with a 6MWT distance of less than 300 metres associated with increase death [9-12].
For assessment of the training effect of EBCR programs, a 6MWT on commencement and completion of the program is advantageous. However, as it is unclear as to what increase in walking distance is considered significant, an accepted term is the ‘minimal clinically important difference’ (MCID) [13-15]. In using the 6MWT as an outcome measure there are two basic questions that must addressed. First, what is the reproducibility of the test and what is considered a MCID difference in metres? Studies have shown that a test-retest difference is of the order of a 7% improvement with the second test done prior to commencement of EBCR [16, 17]. As a commencing 6MWT in EBCR programs is frequently in the range of 350-450 metres, a 7% increase would be of the order of 25-32 metres. Gremeaux et al in a study of 81 patients (95% male, mean age 58.1 years) managed for an acute coronary syndrome determined that the MCID was 25 metres [18], similar to the likelihood of a test-retest result. For other medical conditions (chronic obstructive pulmonary disease (COPD), musculoskeletal pathology), the MCID has ranged from approximately 25-50 metres [19, 20].
Despite extensive investigation of the 6MWT there is limited information defining values based on age and gender which can be applied to the elderly and are relevant to the range of cardiovascular pathology seen in a EBCR program. Equations have been developed based on age, height, weight and gender but there is no general acceptance for reference within position statements by the American Heart Association, American Thoracic Society, European Respiratory Society or the American College of Sports Medicine [19, 21-24]. The purpose of this study was to assess the effect of structured exercise in an EBCR program on 6MWT change and to determine the significance of age, gender, BMI, pathology and exercise attendance on influencing this outcome.
METHODS
Data for this retrospective study was obtained from a client database of a single, stand-alone EBCR facility (Robina) from 2006 and 2018.
Cardiac Rehabilitation Facility
In 2006, the Robina EBCR centre was established by Queensland Health to provide a community facility for comprehensive phase 2 EBCR with a referral source from both public and private hospital and community doctors. Currently it is based in the Robina Precinct, Queensland, Australia.
Patient Recruitment
Patients accepted for the program include acute coronary artery syndromes, cardiac and cardiovascular surgery, intervention for cardiac arrhythmias such as pacemakers, implantable defibrillators, ablation therapy and deconditioning in the presence of known cardiovascular disease. This review process is handled by liaison between EBCR staff and the referring medical practitioner. If the patient is considered as having unstable symptomatic cardiovascular pathology (e.g., chest pain, uncontrolled heart failure, symptomatic arrhythmias and valvular disease) referral is deferred until the medical condition is appropriately managed. Patients with congestive heart failure (CHF) are treated within a separate 12-week program at the Robina rehabilitation facility. Symptomatic comorbidities may limit participation such as osteoarthritis, lung disease, morbid obesity and stroke, but if the EBCR staff believe that benefit can be derived from participation, every effort is made to accept the patient, modifying the exercise prescription to accommodate the disability. As the Robina rehabilitation facility is adjacent to a large public health facility (Queensland Health Robina Hospital), acute medical problems that might occur during patient participation within EBCR can be dealt with promptly.
EBCR Program
Following an initial review and physical assessment of patients in which a detailed description of the program is outlined, patients commence the program once informed consent for exercise participation has been obtained. The program duration is six weeks with a combination of two exercise and educational sessions per week. Both exercise and educational sessions are of a one-hour duration, exercise sessions consisting of a 5-10 minute warm up and cool down period with 40 minutes of multi-station exercise (both aerobic and resistance training). Patients are encouraged to exercise at an intensity of ‘somewhat hard’ i.e., a rating of 3-4 on a modified Borg scale. At the commencement and completion of the six-week program a single 6MWT is undertaken within the complex adhering to the guidelines of the ATS. No attempt was made to determine MCID nor were any health-related quality of life measurements undertaken. The term ‘improvers’ has been used for subjects improving their pre 6MWT distance by either 25 or 50 meters and ‘non-improvers’ for those failing to meet those distances [18-20]. We chose to use the terms ‘improver’ or ‘non-improver’ instead of ‘responder’ and ‘non-responder’ based on a critique by Dolmage et al [25].
Data Collection
Data were recorded directly into an Excel® spread sheet, the format of recorded data undergoing change over the 12-year period. In extracting data from spread sheets, a small number of cells failed to contain information in the nominated format. Where possible this information was sought from available medical records but invariably some data entry could not be recovered. Body mass index (BMI) was mostly recorded as an absolute number though for the year 2007 it was recorded by range (<25, 25.0-29.9, 30-34.9, 35+). Direct recording of BMI on spread sheets was curtailed in 2015, the data used in this study being for the years 2006 to 2014. For all patients the number of exercise and educational sessions were recorded, and the duration of the phase 2 program determined.
Review of the data for analysis and publication was approved by the Human Research Ethics Committee located at the Gold Coast University Hospital.
Statistical Analysis
Categorical variables were expressed as numbers and percentages with continuous variables expressed as mean ± standard deviation. Students paired t test and ANOVA were used to compare 6MWT results for the various categories of age, gender, BMI, attendance and pathology. The distribution of pathological classification groups within EBCR was determined by the chi square test. Statistical calculations were done with inbuilt functions within Excel, Microsoft Office ® and online software, QuickCalcs ® and Astatsa®.
RESULTS
Participants
In this analysis a requirement for inclusion was the completion of a 6MWT on commencement and completion of the phase 2 program. In all, 2524 patients (1923 males, 601 females) met this requirement. A further 792 completed the initial 6MWT only but were excluded from analysis. Patient characteristics are shown in Table 1.

Characteristics of participants
Pathology
In grouping patients by pathology four categories were used; Surgical, Percutaneous Coronary Intervention (PCI), Medical and Other. Surgical patients (n=860, 34.1%) were predominantly coronary artery bypass grafting (CABG), (n=537) and valvular (either alone or in combination with CABG), (n=299). A small number of patients had aortic surgery, heart transplantation and removal of atrial myxomas (n=24). A total of 1189 (47.1%) underwent PCI for acute coronary syndromes (ACS). Medical management with coronary angiography was required for 354 patients (14.0%). A total of 121 patients (4.8%) were classed as ‘Other’, most requiring either ablation or insertion of AICDs (automated implantable cardioverter-defibrillator) for management of cardiac arrhythmias. Pathological classification is shown in Table 2.
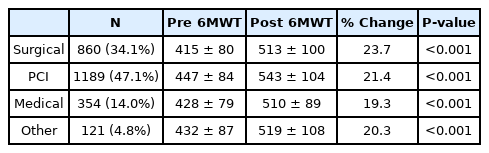
Pathological classification
Age
To determine the effect of age, subjects were stratified into six age ranges of <40, 40-49, 50-59, 60-69, 70-79, 80+years for both males and females as shown in Table 3.
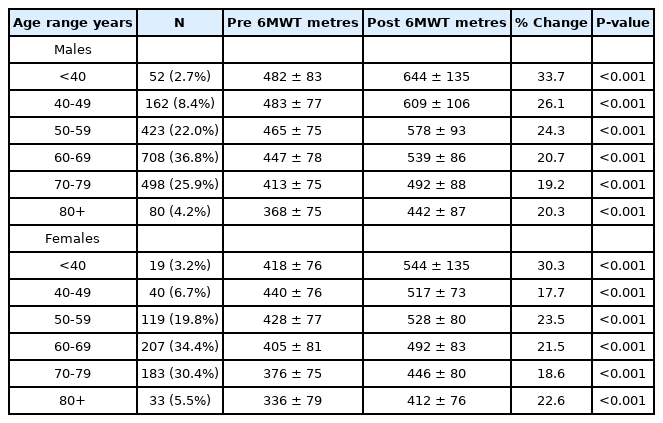
Effect of age and gender on 6MWT results
The post EBCR 6MWT results showed a group mean improvement in excess of 20% for both sexes, an effect strongest in the youngest subjects and observed even in the oldest participants. In considering the age-related effect on the 6MWT, the decline per decade in 6MWT distance does not follow a linear trend. It is less than 20 metres per decade till the sixth decade but from the sixth to the eight decade a more marked decline in distance is observed, with a 40-metre decline noted for both sexes in the eight decade.
Further analysis of the effect of age and gender on the 6MWT result was undertaken by the range of distance covered with the initial pre 6MWT result. Four distance ranges were considered, 1. <300, 2. 300-449, 3. 450-599 and 4. 600+metres. Results for this analysis are shown in Table 4.
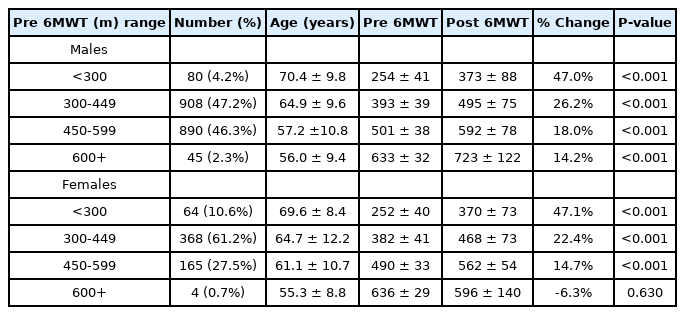
Distance completed with initial 6MWT
In using four categories of distance for the 6MWT (<300 metres, 300-449 metres, 500-599 metres and 600+ metres), an inverse relationship between age and distance covered was evident. Both male and female subjects in the lowest pre EBCR 6MWT distance range (<300 metres) had the highest mean age (males 70.4 ± 9.8 years, females 69.6 ± 8.4 years) and showed the greatest improvement in the post EBCR 6MWT of 47.0% and 47.1% respectively.
Body Mass Index
The effect of body mass index (BMI) with ranges being <25, 25-29.9, 30-34.9 and 35+is shown in Table 5.
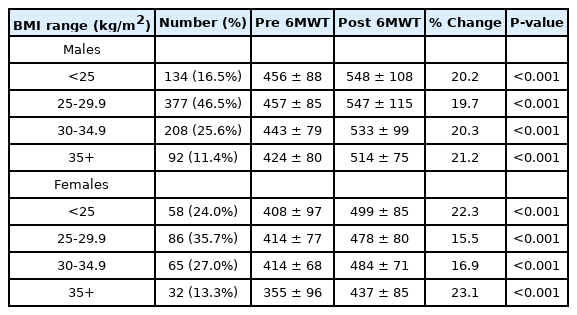
Body mass index
For three of the four BMI categories, <25, 25-29.9, 30-34.9, pre 6MWT were similar for both males and females, with a lower pre 6MWT result in the highest BMI category, 35+. Compared with the <25 BMI category, the 35+BMI category had significantly lower pre 6MWT distances for both males (424±80 metres versus 456±88 metres, p=0.006) and females (355±96 metres versus 408±97 metres, p=0.02). Similar percentage improvements in the post 6MWT were observed for both males and females for the 35+ BMI group (males 21.2%, females 23.1%) compared with the <25 BMI group (males 20.2% and females 22.3%).
Attendance at exercise sessions
Attendance at exercise sessions was considered excellent with 2129 (84.4%) of patients attending for a total of 9 or more sessions of the 12 available sessions. Results are shown in Table 6.
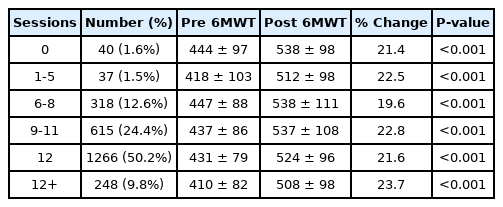
Attendance at exercise sessions
Only 3.0% of subjects attended less than 6 exercise sessions but these two groups (0 sessions, n=40 and 1-5 sessions, n=37) also showed an improvement of greater than 20% in their post 6MWT distance, namely 21.4% and 22.5% respectively. For those with the highest level of attendance (9-11 sessions, n=615, 12 sessions, n=1266 and 12+ sessions, n=248) increases in the post EBCR 6MWT were 22.8%, 21.6% and 23.7% respectively.
Change in 6MWT in response to EBCR
With this community based EBCR program, subjects were reviewed based on whether they were able to improve on the pre 6MWT by either 25 or 50 metres, with results of both male and female patients being shown in Table 7.
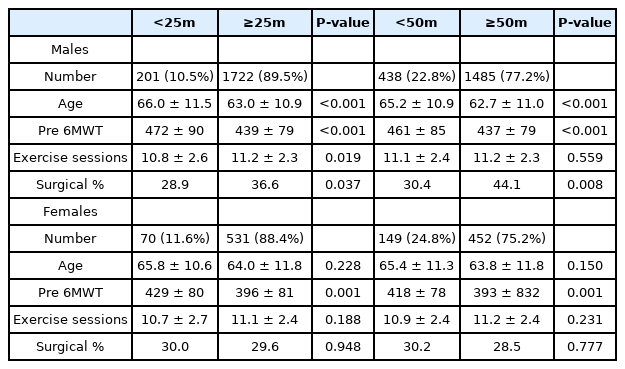
Failure to improve pre 6MWT by either 25 or 50 metres
For a difference of <25 metres between pre and post 6MWT, 10.5% of males and 11.6% of females failed to reach this target, and for a difference of <50 metres this increased substantially to 22.8% for males and 24.8% for females. Based on the failure to improve the 6MWT by these predetermined distances (25 or 50 metres), these subjects were labelled as ‘non-improvers’. Male ‘non-improvers’ for both <25 and <50 metres were significantly older than ‘improvers’ (p<0.001) with a similar, but not significant trend observed with females (<25 metres, p=0.228, <50 metres, p=0.150). For both males and females ‘non-improvers’, there was no significant difference in the number of exercise sessions compared with those exceeding the 25 or 25 metre improvement, the only exception being men with a <25 metre improvement (males <25 metres, 10.8±2.6 sessions, >25 metres, 11.2±2.3 sessions, p=0.019). Using the lower increment of 25 metres, a significantly higher pre 6MWT was attained by both male (p<0.001) and female (p=0.001) ‘non-improvers’ when compared to ‘improvers’. Using the upper increment of 50 metres, the differences between ‘improvers’ and ‘non-improvers’ were also significant for both males (p<0.001) and females (p=0.001).
For males, for both < 25 metre and <50 metre improvement groups, ‘improvers’ were significantly more likely to have had cardiovascular surgery as their pathological classification than the ‘non-improvers’, <25 metre, p=0.037 and <50 metre, p=0.008. This bias towards a surgical classification in the ‘improvers’ was not observed in females.
DISCUSSION
This large retrospective analysis of an EBCR program, a community-based service on the Gold Coast has allowed us to determine what factors may influence the training effect derived from participation in the EBCR program as determined by change in the 6MWT. Because of the large number of patients (n=2524) completing both the pre and post EBCR 6MWT, the effect of age and gender was able to be examined. A similar age-related decline in the pre 6MWT was observed for both sexes with the post 6MWT increasing to a level roughly equivalent to patients two decades younger. The group mean improvement of approximately 20% is in keeping with the finding of other studies [26, 27]. Our study included many subjects 70 years of age and older, with males (n=578) and females (n=216) showing a similar group mean percentage improvement in the post 6MWT of approximately 20%, a finding similar to other studies of the elderly [28, 29]. Importantly, subjects with lowest pre 6MWT distance, the elderly, were able to achieve greater percentage gains in the post 6MWT distance than younger patients. Recognizing the interplay of ageing, sarcopenia and frailty the elderly potentially have the most to gain from participation in EBCR for both maintaining and enhancing physical function which is likely to impact on the quality of daily living [30, 31].
What defines a successful response to EBCR? Is it the level of estimated CRF determined from an exercise test, in this case the 6MWT or the achievement of a defined improvement in walking distance, e.g., in excess of 25 or 50 metres? Or is it just participation in an EBCR program itself?
In achieving a distance improvement of either 25 or 50 metres, we have chosen to use the terminology of ‘improver’ or ‘non-improver’. Dolmage et al has expressed caution in using the terms ‘non-responder’ and ‘non-responder’ [25] as an increase of greater than an MCID may be observed with test-retest variation, even without any intervention, such as EBCR. To label this individual as a ‘responder’ in the absence of participation in an EBCR program is clearly a misnomer, hence our decision to use the alternative labels of ‘improver’ and ‘non-improver’.
Though there was a group mean improvement in the pre and post EBCR 6MWT of 20.9%, should those patients who were unable to reach an improvement target of >25 or >50 metres be arbitrarily labelled as ‘non-improvers’? Approximately one quarter of male (22.8%) and female (24.8%) patients were unable to reach an improvement target of >50 metres. Even with a lesser improvement target of >25 metres as suggested by Gremeaux et al [18], 10.5% males (n=201) and 11.6% of females (n=70) failed to increase their 6MWT by this distance. For these “non-improvers”, whether at a 25 or 50 metre distance, males were significantly older, a similar but non-significant trend being observed in females.
’Non-improvers’ achieved a significantly better pre 6MWT distance than ‘improvers’ in the <25 metre and <50 metre categories for both males (33 metres, p<0.001 and 24 metres, p<0.001, respectively) and females (33 metres, p=0.001 and 25 metres, p=0.001, respectively). The reason for this discrepancy is uncertain. Men, within the ‘improvers’ group were more likely to have had recent cardiovascular surgery as their classification for EBCR.
Recent cardiovascular surgery may impose some limitation on physical performance necessary to perform the 6MWT on entry into the EBCR program, being less likely to impact on the 6MWT performed on completion of the program. However, this feature was not observed with females. ATS guidelines suggest a standardised encouragement protocol as the effect of encouragement can significantly influence the distance achieved with the 6MWT [32]. With encouragement, the Guyatt et al study demonstrated a distance improvement of 30.5 metres, approximately an 8% increase from the initial 6MWT in 43 patients with chronic obstructive pulmonary disease and chronic heart failure [32]. In the Robina program, 6MWT supervision was undertaken by a variety of trained personnel, namely exercise physiologists, nurses and physiotherapists. Their skills in eliciting patient response to the 6MWT may be different and may account for the difference observed in the Robina study. ATS guidelines recommend the use of an absolute value of 6MWT change but as our results indicate, improvement in the 6MWT is affected by both age and sex [1]. Accordingly, it may be more appropriate to use a “variable” value such as a percentage increase in walking distance.
The training response related to pathological classification shown by an increase in 6MWT distance was highest for surgical patients (23.7%) when compared with PCI (21.4%) and medical management (19.3%). In our study, the mean pre 6MWT distance for surgical patients was 8% lower than that of PCI patients (surgery 415 ± 80 metres, PCI, 447 ± 84 metres, p<0.001) similar to results reported by Jelinek and Izawa [33, 34]. Obesity did not adversely affect the training response of the 6MWT with EBCR. Both males and females with a BMI 35+ recorded the highest percentage increase in 6MWT distance (20.2% and 22.3% respectively). In a 3 month (36 sessions) EBCR program, Lavie et al has reported a 24% increase in exercise capacity measured in METs, this improvement in cardiorespiratory fitness being accompanied by a small but significant reduction in BMI from 31.2 to 30.2 (p<0.0001) [35].
Only 77 (3.0%) patients attended less than 6 of the 12 available exercise sessions but demonstrated comparable post 6MWT distance improvement to those with higher levels of attendance at exercise sessions. Ades et al reported a similar finding noting no apparent relationship between the number of exercise sessions attended and the improvement in the post 6MWT [30]. This observation may be explained by home based activity performed by those with no or low attendance rates as physical activity performed outside of the Robina EBCR unit was not recorded but was encouraged.
Tests that quantify cardiorespiratory function assist with prognostication of long term morbidity and mortality [36]. Higher levels of CRF in both the healthy and those with coronary artery disease are associated with reduced mortality [36, 37] and participation in EBCR following PCI is associated with reduced mortality rates [38, 39]. The usefulness 6MWT as a prognostic variable is dependent on its relationship to VO2.
In performing a 6MWT most healthy adults will be limited to a maximal walking speed of about 7 km/h, above which a transition to jogging will take place [40]. For individuals who are not aerobically limited by dyspnoea at this walking speed, the limitation of the 6MWT is one of gait mechanics. Equations of varying complexity using height, weight, age and gender have been determined for the prediction of VO2peak from the 6MWT for both healthy subjects and those with cardiorespiratory disease [7, 19, 21-23] . However, these equations are rarely used to estimate CRF in research studies utilizing the 6MWT. By comparison, subjects with severe heart failure frequently have a maximum 6MWT distance of less than 300-400 metres, the limitation being due cardiorespiratory factors. More recently, Ross et al published a simplified equation with the only variable being 6MWT distance in metres, the equation being mean VO2peak (mL·kg·min-¹) = 4.948 + 0.023 * mean 6MWD (metres) [7]. A caveat on the use of the Ross equation is that it should only be used with a VO2peak less than 20 mL·kg·min-1 or with a 6MWT distance less than 600 metres.
Prediction of CRF is commonplace when using maximal cardiopulmonary exercise testing (CPET) utilizing equations based on treadmill speed, incline or protocol time, the most common reference set being in ACSM publications [41]. Can cardiovascular studies using either a 6MWT or CPET be compared for prediction of morbidity and mortality outcomes, using the exercise test result to determine CRF? Martin et al in reporting on mortality after contemporary EBCR used treadmill testing to determine predicted VO2peak in 5641 patients (mean age 60.0 ± 10.3 years, males 76%) with known CAD [42] . The equation used for prediction of VO2peak compensated for handrail support during testing [43]. Patients in that study were graded into 3 categories, low fitness (<5 METs), n=424 (7.5%), moderate fitness (5-8 METs), n=2,475 (43.9%) and high fitness (>8 METs), n=2,742 (48.6%). In the Robina study of 2524 patients, 1902 (92.2%) patients had a pre 6MWT of less than 546 metres and would have been classed as low fitness (<5 METs) based on VO2peak determined from the Ross equation. The remaining 162 (7.8%) patients would have been classed as having moderate fitness (5-8 METs, i.e., 546-600+ metres), a totally different profile with much lower predicted estimates of CRF compared with the Martin et al study [42]. Otherwise, the comparison of the studies shows quite a similar patient profile based on age and sex (Robina study - mean age 63.4 ± 11.0, males 77%) and underlying cardiac pathology. This study comparison highlights the known difficulty in using predicted levels of VO2peak because of the unacceptably large errors of prediction, in excess of 20% [44, 45].
If EBCR participation translates into a subsequent long-term increase in physical activity, this is clearly an important benefit of EBCR. In an analysis of physical activity and mortality in patients with stable coronary artery disease by Stewart et al [46], a progressive decrease in mortality was associated with increased habitual activity, this effect being greatest with people commencing even small amounts of activity such as walking for 100 minutes per week, equivalent to 5 MET hours per week. Whilst this is less than the general recommendation of 150 minutes of moderate physical activity (3-6 METs) or 75 minutes of vigorous physical activity (6+ METs), lower amounts of physical activity can still confer significant benefit [47]. The ability to measure daily physical activity has been made possible by the sophisticated technology of wearables (smart watches). A recent study showed a significant association between increased levels of daily physical activity and higher levels of 6MWT distance [48]. In the context of comprehensive EBCR, factors other than improved CRF and increased physical activity may reduce mortality and morbidity due to improved cardiac risk factor control and compliance with medication [49].
CONCLUSIONS
In conclusion, The 6MWT is widely used in EBCR as it is a safe and simple test to perform. Despite a plethora of publications containing age and gender-based values for normal and disease states, no equation is commonly used for defining CRF for the 6MWT, a necessary measurement for prognostic studies of morbidity and mortality for cardiorespiratory disease. While distance walked may have prognostic significance, it is most relevant to distances of less than 300-350 metres, associated with severe (and often end-stage) disease, a distance well below that achieved by most patients who routinely attend EBCR programs. For CR participants who are asymptomatic (NYHA I and II) and able to complete distances greater than 400-500 metres, suitable data for prognosis based on 6MWT distance is lacking. Nor is there any accepted conversion of longer distances e.g., greater than 500-600 metres into VO2peak (commonly expressed as METs) to allow comparison with maximum stress test data, whether from cycle ergometry or treadmill testing. Our study questions the value of MCID in an asymptomatic population (intentionally excluding CHF), which with exercise training is likely to achieve a VO2peak within a normal range for age.
The 6MWT is perceived as an exercise test by EBCR participants, the aim of structured exercise being to improve their pre-CR 6MWT result. It is a submaximal test for those without a cardiorespiratory limitation which limits its prognostic value. However, the 6MWT acts as an incentive to achieve an improvement in distance, a surrogate measure of improved CRF. This observation is particularly relevant for the elderly who stand to derive major benefit from participation in EBCR.
Acknowledgements
The authors would like to acknowledge all Queensland Health staff who participated in patient assessment and management since the commencement of EBCR on the Queensland Gold Coast. The authors are indebted to Professor Neil Oldridge (College of Health Sciences, University of Wisconsin, Milwaukee, USA) for his critique of the manuscript and the staff of the Gold Coast University Hospital for their invaluable assistance in sourcing reference material.
Notes
Conflict of Interest
The authors declare no conflict of interest.