Children with Cardiomyopathy have Active Lifestyles Despite Reporting Disease-Specific Barriers to Physical Activity: A Mixed-Methods Study
Article information

Abstract
OBJECTIVES
This exploratory mixed-methods study explored the barriers to physical activity, daily physical activity and submaximal exercise capacity among children with and at risk for cardiomyopathy and children with atrial septal defects.
METHODS
The study followed a convergent parallel mixed methodology design. Semi-structured interviews explored physical activity barriers. Seven-day accelerometry assessed moderate-to-vigorous physical activity, and an intermittent cardiopulmonary exercise test measured submaximal exercise capacity.
RESULTS
Twenty children, including 5 with cardiomyopathy (n=2 females, 14.2 ± 2.7 years old), 7 who were genotype-positive phenotype-negative for cardiomyopathy (n=5 females, 10.6 ± 3.3 years old) and 8 with atrial septal defects (n=4 females, 9.4 ± 3.8 years old) were recruited. Children with cardiomyopathy reported disease-specific physical activity barriers, while children who were genotype-positive phenotype-negative perceived barriers related to lack of time, parent support or activity motivation. The average daily moderate-to-vigorous physical activity was less than the recommended 60-minutes/day (n=20, mean 48.1 ± 18.0 minutes). Children with cardiomyopathy participated a median of 141.2 [interquartile range (IQR): 98.8) minutes of light-intensity physical activity and a median of 55.6 (IQR: 34.6) minutes of moderate-to-vigorous physical activity. The average submaximal exercise capacity was low (n=16, 25.2 ± 5.7 mL/kg/min). Estimated submaximal exercise capacity, including metabolic equivalent (4.5 ± 3.1 METs), respiratory exchange ratio (median = 1.0, IQR: 0.09) and ratings of perceived exertion (median = 7, IQR: 5) at peak exercise suggest that children with cardiomyopathy appear to have the exercise capacity to participate in low-to-moderate intensity activities.
CONCLUSIONS
These novel data suggest that a diagnosis of cardiomyopathy may not preclude children from participating in a healthy, active lifestyle. However, they perceive disease-specific physical activity barriers and may require support to optimize their level of participation for optimal health.
INTRODUCTION
Pediatric cardiomyopathies are rare diseases of the cardiac muscle affecting approximately 1 in every 100,000 children [1]. With childhood cancer survivors at a 15-fold increased risk of developing cardiomyopathy and heart failure than age-matched controls [2], the number of children affected by cardiomyopathy is anticipated to rise substantially [3]. Children with cardiomyopathy are also at high risk for poor health outcomes, including cardiovascular abnormalities, arrhythmias, heart failure and sudden cardiac death [1,4,5]. With the rising prevalence of pediatric cardiomyopathies [1], exploring avenues to enhance health-promoting behaviours, like physical activity and exercise, to improve positive health outcomes is greatly needed. Current expert consensus physical activity guidelines recommend individuals with cardiomyopathy avoid high-intensity physical activity [6]. Physician-guided restriction has resulted in unique barriers to physical activity among adults with cardiomyopathy, including purposeful reduction or withdrawal from activity [7]. As a result, individuals with cardiomyopathy are at high risk for inactivity-related morbidities, low fitness levels [8], reduced health-related quality of life and psychological well-being, and atherosclerosis, hypertension, and diabetes [1,7,9-11].
Although adult physical activity studies are available [11], the physical activity behaviours of children with cardiomyopathy have not been explored. It is currently unknown whether children with cardiomyopathy have adequate exercise capacity for physical activity or experience barriers that restrict their physical activity participation. This knowledge gap may lead clinicians to be overly conservative when advising children with cardiomyopathy about exercise. Whether parents, teachers or the children themselves would limit their physical activity participation is also unknown. Identifying children at risk for inactivity and promoting healthy behaviours early in childhood may lead to positive health outcomes and could potentially halt the detrimental cycle of inactivity seen among adults with cardiomyopathy.
Therefore, this exploratory mixed-methods study had three objectives. The primary objective of this study was to qualitatively explore the physical activity barriers reported by children with and at risk for cardiomyopathy [defined as children who are genotype-positive phenotype-negative (G+P-)]. The secondary objectives of this study were to quantitatively measure and describe the a) daily moderate-to-vigorous activity physical activity (minutes) using 7-day accelerometry and b) submaximal aerobic exercise capacity, defined as the oxygen consumption (mL/kg/min) required at a heart rate of 150 beats per minute. These quantitative variables were contextualized with a reference group of children with simple atrial septal defects (ASD) that should not have activity limitations.
METHODS
This cross-sectional study followed a convergent parallel mixed methodology design. Qualitative and quantitative data were collected in parallel, analyzed separately and then merged to form conclusions about the physical activity behaviors of children with cardiomyopathy. The Guidelines for Conducting and Reporting Mixed Research were followed [12]. This study was approved by the Children’s Hospital of Eastern Ontario Research Ethics Board (Ethics file #17/189x) and the University of Ottawa Research Ethics Board (Ethics file: H-04-18-461). All participants and their parents gave written informed assent and/or consent to participate.
Participant Recruitment and Eligibility
Pediatric cardiology patients from the Children’s Hospital of Eastern Ontario, between 5 and 17 years old, were screened for study eligibility through physician caseload and medical chart review. Children were included in the study if they had a medical diagnosis of a) cardiomyopathy (e.g., hypertrophic, dilated or chemotherapy-induced cardiomyopathy); b) G+P- for cardiomyopathy; or c) repaired ASD or ASD not requiring treatment. Participants with ASD were enrolled as a reference population of children whose physical activity was expected to be unaffected by the cardiac diagnosis. However, similar to the cardiomyopathy patients, they have a cardiac diagnosis and are followed in a cardiac clinic. Participants were excluded if they had a) physical activity contraindications preventing study participation as determined by the treating cardiologist, b) had a syndrome, non-cardiac medical condition or disability known to influence physical activity or motor skill development (e.g., cerebral palsy, Down syndrome) or c) if they underwent cardiac surgery or catheterization intervention within the preceding 6 months. Eligibility was confirmed by the responsible cardiologist.
Semi-structured interviews
A phenomenological approach with thematic inductive analysis [13] was used to explore participants’ perceived barriers to physical activity. Since activity barriers are known for pediatric patients with congenital heart defects (including ASD) [14], only participants diagnosed with cardiomyopathy or at risk for cardiomyopathy completed the semi-structured interview component of this research. The interview guide consisted of a mixture of open- and closed-ended items and be seen in Supplementary Material. KM conducted all 12 interviews, either before or after the submaximal exercise test, in a private room in the cardiology clinic. All interviews were audio-recorded and then transcribed verbatim for analysis.
Accelerometry
Participants were asked to wear an Actical Z-series accelerometer (Philips Respironics, Murrysville, Pennsylvania) above the right iliac crest at the mid-axillary line for 7 consecutive days [15]. Accelerometer data were recorded in 15-second epochs and established cutpoints were used to calculate minutes of light, moderate-to-vigorous, and total physical activity performed per day [16]. Accelerometry data were considered valid and included in the analysis if participants wore the Actical for at least 3 weekdays and 1 weekend day [15] with at least 10 hours of Actical wear time each day [17]. To account for participant wear time variability, time spent in each physical activity category (i.e., light, moderate-to-vigorous, and total physical activity) per day was calculated as (5 days × Average weekday physical activity) + (2 days × Average weekend day physical activity)/7 days.
Submaximal exercise capacity test
Participants completed an intermittent submaximal cardiopulmonary exercise treadmill assessment that was designed using the submaximal stages of the Bruce protocol [18,19]. Body mass (kg) and height (cm) were measured. Participants were fitted with a 10-lead electrocardiogram (CASE 8000; GE Medical Systems, Milwaukee, Wisconsin), blood pressure cuff (FlexiPort re-usable blood pressure cuff; Welch Allyn, Skaneateles Falls, New York) and a fitted rubber mouthpiece for breath-by-breath indirect measures of oxygen consumption (VMAX Encore Metabolic Cart, Sensormedic, San Diego, California). Baseline heart rate, blood pressure, oxygen consumption, and respiratory exchange ratio were measured while the participant was seated comfortably for 10 minutes or until the respiratory exchange ratio stabilized between 0.67 and 1.00 [19].
A 2-minute warm-up stage (6% grade at 1.0 mph) familiarized participants with treadmill walking and the monitoring equipment. Participants then completed a minimum of three 5-minute bouts of exercise at workloads designed to achieve 40%, 60%, and 80% of their estimated maximum heart rate. The rest period between exercise bouts continued until the heart rate returned to 10% of the resting value. A standard 10-lead electrocardiogram and respiratory variables were monitored throughout the test and with blood pressure and rating of perceived exertion (Borg 1-10 Scale) [20] collected at the end of each exercise stage. For the cool down, the treadmill speed and incline were gradually decreased to the warm-up stage for 2-minutes.
Data Analyses
Descriptive statistics were performed to describe demographic information and quantitative outcomes by study group as means ± standard deviation or medians [interquartile range, (IQR)] for normally and non-normally distributed data, respectively, and frequencies (n, %) for categorical data. The Shapiro-Wilk test was conducted to determine the distribution of each variable. Given the exploratory nature of this study and the lack of physical activity research in pediatric cardiomyopathy, we did not have effect estimates to conduct formal sample size calculations. Thus we did not perform hypothesis testing or set a pre-specified significance level. All descriptive analyses were performed using Stata 16.1 (2020; StataCorp LP, College Station, Texas).
Interviews were inductively analyzed by KM using the six steps described by Braun and Clark [13]. Data familiarization occurred as the data were transcribed verbatim and through reading and re-reading the transcripts. Codes were identified across each data set, with the data from one participant analyzed at a time. Once all interviews were coded, themes were developed by ordering and refining the identified codes into lower-level and higher-level themes. Finally, themes were named and defined, and the most relevant quotations were chosen to exemplify each theme. NVivo 12 (QSR International, Burlington, Massachusetts) was used to assist with interview coding and data management.
Light physical activity was defined as less than 375 counts per 15-second epoch, and moderate-to-vigorous physical activity was defined as at least 375 counts per 15-second epoch via an accelerometer [16]. Total physical activity was calculated as the sum of all physical activity counts. Submaximal aerobic exercise capacity was defined as the oxygen consumption required when exercising at a heart rate of 150 beats per minute. It was estimated by extrapolating or interpolating the heart rate-oxygen consumption linear relationship to a standardized value of 150 beats per minute. Metabolic equivalents (METs) at 150 beats per minute were calculated by dividing mean oxygen consumption at 150 beats per minute by the resting metabolic rate, which was estimated using the sex-specific Schofield equations [21].
RESULTS
A total of 45 potential participants were identified through medical chart review, of which 40 met eligibility criteria (9 cardiomyopathy (n=5 hypertrophic, n=3 dilated, n=1 chemotherapy-induced); 11 G+P- for cardiomyopathy; 20 ASD). Patients were excluded because physical activity was contraindicated (n=2), patient status was unknown (n=2), or the physician refused to approach the patient for participation in research (n=1). Twenty individuals did not participate (n=13 declined, n=6 unable to contact, n=1 withdrew). The study flowchart is presented in Figure 1.
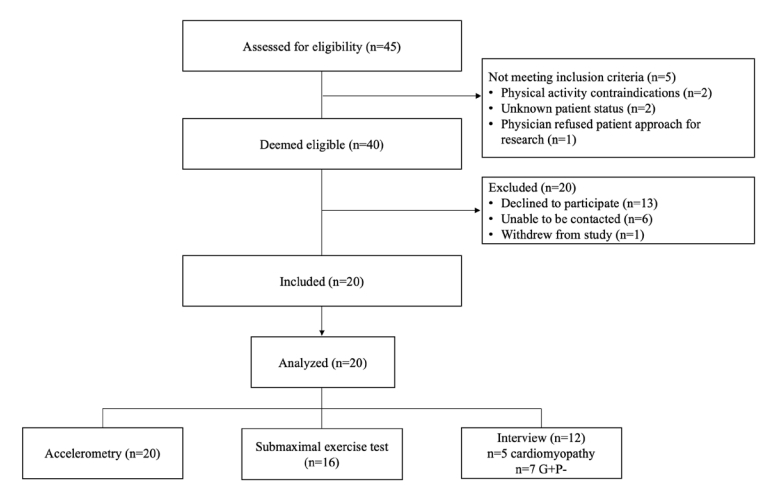
Participant flow chart.
G+P-: genotype-positive phenotype negative
Participant Characteristics
Table 1 summarizes the characteristics of the 20 participants included in the analysis, disaggregated by study group. Twenty participants (55% female, mean age 11.0 ± 3.8 years) were included in our analyses. In the cardiomyopathy group, participants were diagnosed with dilated (n=2, 40%), hypertrophic (n=2, 40%) or cancer-related cardiomyopathy (n=1, 20%). Participants with cardiomyopathy had a median ejection fraction of 65% (IQR: 26), while participants who were G+P- for cardiomyopathy and ASD had a median ejection fraction of 70% (IQR: 5), 73% (IQR: 7), respectively. Two participants with cardiomyopathy (n=1 hypertrophic, n=1 dilated) were restricted from participating in competitive sports. One participant with cardiomyopathy (n=1 hypertrophic) had a prosthetic leg, but this did not restrict or limit safe physical activity participation. Two participants were prescribed cardiovascular medication (1 beta-blocker, 1 angiotensin-converting enzyme-inhibitor). Non-cardiac conditions were present in 6 participants (n=4 cardiomyopathy, n=1 ASD, n=1 G+P- for cardiomyopathy), including respiratory (n=2), digestive (n=2), cancer (n=1) and attention deficit hyperactivity disorder (n=1).
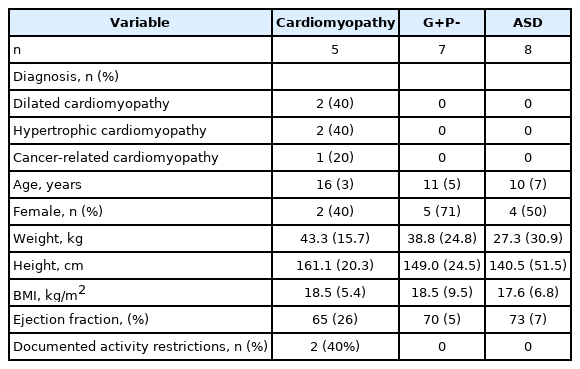
Participant characteristics disaggregated by study group.
Physical Activity Barriers
Twelve participants (n=5 cardiomyopathy and n=7 G+P- for cardiomyopathy) completed semi-structured interviews, which lasted between 10 and 33 minutes (mean=13.4 ± 8.0 minutes) and generated 37 pages of transcripts. The main themes identified during the semi-structured interviews were “influences of the disease” and “psychosocial influences” (Figure 2).
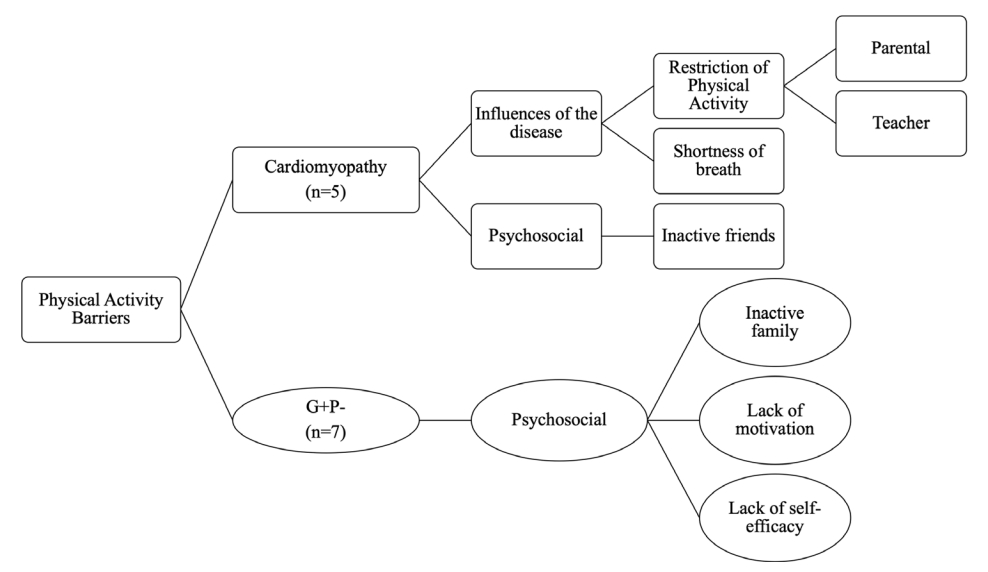
Physical activity barriers by study group
Data have been presented as keywords among themes developed during the thematic analysis for both study groups. Abbreviation: G+P-, genotype-positive phenotype-negative.
Influences of the Disease
Both participants with cardiomyopathy and their parents described parent-initiated physical activity restrictions. “My mom doesn’t let me do certain activities… she always makes me bring the defibrillator” (HCM 7). “His dad also has hypertrophic cardiomyopathy, and so when the whole family is planning an activity, we choose safer sports, but it is more restricted than it usually is with just him” (Parent HCM 1). When asked about allowing sports with friends, Parent HCM 2 responded: “I would allow it, but his mom wouldn’t let him because of the fear that many things can go wrong.”
Participants with cardiomyopathy also described teacher-imposed physical activity restrictions. “For school, we needed to complete a 5km run… it was worth 10% of my mark depending on the times that we got on the run. I was advised to try and pick something else to do” (DCM 9). “Well, my teachers encourage me to not be active” (HCM 7). “My teacher last year said I couldn't play soccer because of physical reasons... I haven’t played soccer at school ever since” (HCM 11). One participant (CCM 22) indicated that her participation was limited because teachers could not adapt the classes to her abilities. “I got all my gyms exempted because the teachers couldn't adapt gym class to me. They recommended that I sit down because I couldn't run a 5km run. I understand that it is extremely unrealistic. I have tried before, like I've run a 2km, but I stopped halfway because I couldn't continue anymore. So, I guess, not being able to adapt the activities to me”.
Most participants with cardiomyopathy found breathlessness was a common barrier to activity participation. “I find I get short of breath very easily, so much that I feel that sometimes I walk up the stairs and feel like I need to stop walking” (CCM 22). “There are times when we go for bike rides, and sometimes he just can’t make it home… because he is too tired” (parent HCM 1). They also recognized the limitations imposed by their physical abilities. “I used to play soccer, and I would love to play volleyball, but it doesn’t seem reachable for me from a physical perspective… I was playing volleyball with my friend, and she was trying to show me the basics, and I was like, this is impossible for me” (CCM 22).
Psychosocial Influences
Participants who were genotype-positive but phenotype-negative for cardiomyopathy described their parents and family as inactive, indicated that they do not like to be active or prefer to choose sedentary activities, or that their parents are too busy to do activities with them. They said, “At home, we play board games… We watch movies together. When we have nothing to do, we are just sitting there on the couch to read and watch something” (G+P- 8). “Sometimes they have work to do and are busy and stuff” (G+P- 1). “Yes, my mom can't run and my dad… probably can't run either. Well, my mom can run, she just doesn't like it… and well my dad works all weekdays” (G+P- 6). One participant reported being active with his family, “I like to jump on my trampoline with everyone” (G+P- 2).
These participants also identified a lack of motivation or limited self-efficacy as barriers to physical activity. “Sometimes I don’t have enough energy at the end of the day… I would rather play video games than go outside, I like to play a lot of card games on my tablet” (G+P- 6). “My parents wanted me to go on a competitive team, but I wasn’t ready to move up to competitive, so I decided to stop altogether” (G+P- 1). “My friends are big risk-takers like they do hip-hop and gymnastics. They'll do backflips and wheelies on their bikes, and I'll just watch and bike around. I can't do that stuff.” (G+P- 5). Participants with cardiomyopathy indicated that their friends were not very active, often describing a lack of time or rough play as making it difficult to participate. “My friends aren’t very active… we don’t have much time to be active” (DCM 9). “I don’t like playing soccer at school because sometimes kids are a bit rough, so I play three squares with my friend”(HCM 11).
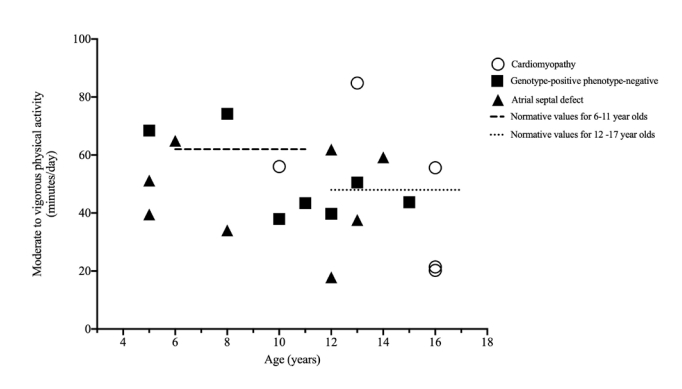
Accelerometry
Table 2 displays the physical activity data, disaggregated by study group. All 20 participants had valid physical activity data. Participants performed an average of 48.1 ± 18.0 minutes of moderate-to-vigorous physical activity per day. Five participants (n=5/20, 25%; n=1 cardiomyopathy, n=2 G+P-, n=2 ASD) achieved the recommended average of 60 minutes of moderate-to-vigorous physical activity per day [22] (Figure 3), a proportion that is not significantly different from the 33% of Canadian children who achieve this standard (z=0.77, p=0.23) [23]. Children with cardiomyopathy performed a median of 55.6 (IQR: 34.6) minutes of moderate-to-vigorous physical activity, while children who are G+P- for cardiomyopathy and ASD performed a median of 43.7 (IQR: 30.5) minutes, and 45.4 (IQR: 24.8) minutes of moderate-to-vigorous physical activity, respectively. In total, the cardiomyopathy group performed a median of 161.4 (IQR: 109.2) minutes of total physical activity per day, while the G+P- and ASD groups performed 164.7 (IQR: 97.9) and 225.3 (121.9) minutes of total physical activity per day, respectively.

Physical activity data disaggregated by study group.
Submaximal Aerobic Exercise Capacity
Table 3 displays the exercise testing data, disaggregated by study group. Fifteen participants (n=4 cardiomyopathy, n=4 G+P- for cardiomyopathy, and n=7 ASD) had valid submaximal aerobic exercise capacity measures. Two participants (1 male G+P- for cardiomyopathy, 1 female with ASD) refused to wear the exercise monitoring equipment, two participants (female who was G+P- for cardiomyopathy) had scheduling conflicts, and one (female chemotherapy-induced cardiomyopathy) had a change in medical status, making the participant ineligible for exercise testing. Individuals with cardiomyopathy had a median submaximal exercise capacity of 24.6 (IQR: 13.9) mL/kg/min. In contrast, participants with G+P- for cardiomyopathy and ASD had a median submaximal exercise capacity of 23.9 (1.4) mL/kg/min and 26.4 (5.1) mL/kg/min, respectively. At peak exercise, children with cardiomyopathy achieved a mean VO2peak of 29.0 ± 11.1 mL/kg/min, while children who are G+P- for cardiomyopathy and ASD achieved a median VO2peak of 28.7 (IQR: 1.0) 1 mL/kg/min and 32.2 (IQR: 11.6) 1 mL/kg/min, respectively. No adverse events occurred during the submaximal exercise tests, suggesting that our incremental protocol targeting 40 to 80% of the estimated maximal heart rate was safe and feasible in this population of children.
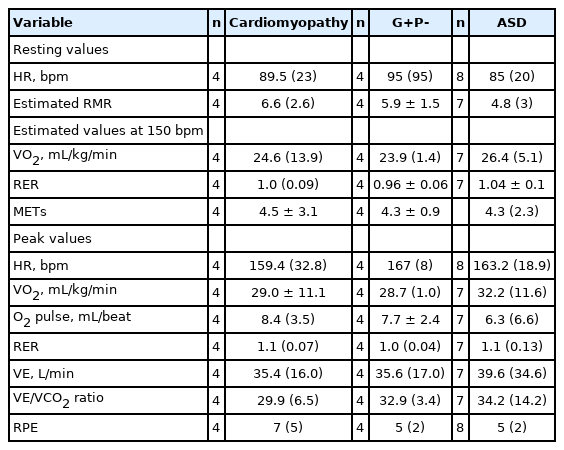
Exercise testing data disaggregated by study group.
DISCUSSION
This study uniquely explored the physical activity barriers, behaviours and submaximal exercise capacities in a convenience sample of children with or at risk for cardiomyopathy. We found that children with cardiomyopathy or who carry a genetic risk for cardiomyopathy have activity levels and submaximal exercise capacity similar to children with ASD. Children with cardiomyopathy report their physical activity is often restricted by responsible adults (e.g., parents, teachers). While children with cardiomyopathy focus on disease-specific barriers and activity limitations, children with a genetic risk for cardiomyopathy (e.g., G+P-) emphasize psychosocial barriers, such as limited motivation or self-efficacy. Findings from submaximal exercise testing help support these identified barriers. Children with cardiomyopathy report greater ratings of perceived exertion during submaximal exercise testing than those with G+P- for cardiomyopathy.
Our participants with cardiomyopathy reported various physical activity barriers, including parental and teacher restriction, fear of injury, shortness of breath and lack of self-efficacy for physical activity that can hinder physical activity participation. These findings align with previous research among children with congenital heart defects, who often report low levels of self-efficacy and perceived confidence for physical activity [24-26]. Parental overprotection and exclusion by teachers are also prominent barriers for children with congenital heart defects [24,25]. Interventions that target barriers to participation in physical education classes should be evaluated, given the physical, psychological, and social health benefits of school-based activity [27].
The barriers described by children with cardiomyopathy often focused on the influence of their disease (e.g., overprotection, shortness of breath). These barriers are consistent with the barriers reported by adults with hypertrophic cardiomyopathies, such as “I was advised not to exercise” or “I might get injured or damage my health” [11]. These disease-focused barriers were not reported among our G+P- participants who are currently healthy. They focused on psychosocial barriers such as lack of motivation, having an inactive family, and a lack of time for physical activity, which are consistent with the barriers to physical activity among healthy youth [28,29]. These data suggest that their gene-positive status does not significantly impact their approach to physical activity. Our study results indicate that children with cardiomyopathy and their families identify barriers unique to their medical condition. Future work should explore targeted physical activity interventions to support a physically active lifestyle.
Daily moderate-to-vigorous physical activity levels were similar across study groups, a finding consistent with research suggesting that congenital heart defect diagnosis [30] or severity [26] are not associated with habitual physical activity. Mean daily moderate-to-vigorous physical activity found in the present study (48.1 minutes/day) is also consistent with previous reports (49 minutes/day) among children with congenital heart defects or cardiac transplants [26], suggesting that our sample, although small, may be representative of this population. Although children with cardiomyopathy may have physical activity levels similar to other pediatric cardiac patients [31,32], their tendency to perform limited moderate-to-vigorous physical activity may result from their disease-focused barriers to physical activity. Nonetheless, it is promising that we observed that children with cardiomyopathy achieved a median 141.2 (IQR: 98.8) minutes of low-intensity physical activity, suggesting adherence to published physical activity guidelines [6]. An important avenue for future research could focus on exploring their perceived facilitators for physical activity and whether they can be utilized to develop effective behaviour change strategies specifically for children with cardiomyopathy.
We found that 25% of participants (n=5) met the current moderate-to-vigorous physical activity recommendation of 60 minutes per day [22]. The percentage is low but consistent with data for Canadian children (33% meet the guideline) [23]. The percentage of adults meeting the recommended level of physical activity (150 minutes per week) is also similar among those with (12%) [11] and without (15%) [17] cardiomyopathy. That 75% of pediatric cardiomyopathy patients are less active than recommended is of concern and suggests they are at increased risk for morbidities associated with inactivity (e.g., cardiovascular disease, diabetes). Unfortunately, these negative health consequences may be magnified among children with cardiomyopathy whose cardiac function is already impaired. Given the similarity in physical activity participation among our study participants and healthy Canadian children [23], our preliminary data provides some evidence that children with cardiomyopathy may be just as likely as healthy children to move into a “cycle of inactivity” as they get older. Therefore, there is a clear need to increase our knowledge within this important research area and understand whether addressing the identified barriers through targeted interventions can optimize the physical activity behaviours and health outcomes of children with cardiomyopathy.
We examined submaximal exercise capacity among children with cardiomyopathy to measure the cardiopulmonary fitness relevant to daily activity [33], including physically active play with peers. Our cardiomyopathy participants achieved an estimated 4.5 ± 3.1 metabolic equivalents (METs) at a heart rate of 150 beats per minute. Since moderate physical activity is defined as requiring 3-6 METs [6] or activities producing a heart rate of 140-160 beats per minute [34], children with cardiomyopathy appear to have the capacity for light-to-moderate intensity activities (e.g., hiking, swimming, doubles tennis, Frisbee, catch) [35]. This finding contrasts with published recommendations that limit most moderate-intensity activities [6]. However, our participants reached a median respiratory exchange ratio of 1.1 (IQR: 0.07) and reported a median RPE of 7 (IQR: 5) while exercising at peak exercise. These findings highlight that our cohort of children with cardiomyopathy may perform at near maximal exercise capacity during daily physical activity, suggesting that they may not sustain this activity level for long periods. Nonetheless, our findings provide the first objective measurements of exercise capacity in children with cardiomyopathy. Future research should explore the effect of personalized exercise prescription on physical activity behaviours in this population of children.
Understanding the submaximal exercise response in children with cardiomyopathy can provide novel information regarding their capacity to perform everyday physical activity. The Youth Compendium of Physical Activities [35] provides the metabolic equivalents required for various sports and games. Research is needed to evaluate if matching submaximal exercise test results from children with cardiomyopathy to Compendium activities can enable clinicians to mitigate activity uncertainty and reassure patients and their families about the child’s ability to be physically active [36]. An important future research direction is determining the clinical utility of submaximal exercise testing and identifying clinically feasible methods for accurately assessing activity participation. Furthermore, such empirical data could help provide a foundation for evidence-based expert consensus physical activity guidelines for children with cardiomyopathy.
Strengths and limitations
Exercise recommendations for children with cardiac diagnoses are often extrapolated from maximal cardiopulmonary exercise test results [37]. A strength of the present study was using an intermittent submaximal exercise protocol to measure the exercise capacity required for everyday activities [33]. Physical activity barriers were identified using semi-structured interviews, enabling participants to discuss and elaborate on their physical activity perspectives. The mixed-methods approach, which combined quantitative measures of physical activity and exercise capacity with qualitative data on physical activity barriers, provided a more holistic perspective of the physical activity capacity and behaviors of children with cardiomyopathy.
A limitation of the current study was the small sample size. This study was exploratory in nature and is the first to explore the barriers to physical activity, physical activities, and exercise capacities in a convenience sample of children with cardiomyopathy. All eligible cardiomyopathy (n=9) and genotype-positive but phenotype-negative for cardiomyopathy (n=9) patients from a single institution were contacted to participate, and 67% enrolled, providing a reasonable sample of this rare population (1 in every 100,000 children). In the future, multi-site collaboration is encouraged to capture a more extensive and diverse sample of children with cardiomyopathy. Furthermore, more female patients tended to decline participation, and the cardiomyopathy patients tended to be older, which may have influenced our results. Since physical activity is expected to decrease with increasing age, and results between our study groups were similar, the cardiomyopathy participants who enrolled may have been more active than those who declined participation. During submaximal exercise testing, children were allowed to hold onto the guard rails, which could have reduced the metabolic cost of the work produced [18]. We estimated the resting metabolic rate using the Schofield equations [21], which may have impacted the calculation of metabolic cost.
CONCLUSIONS
In conclusion, our exploratory study offers preliminary data on the physical activity and exercise capacity of the unique population of children with or at risk for cardiomyopathy from a single institution. We found that despite reporting disease-specific physical activity barriers, the results of this study suggest that children with cardiomyopathy have sufficient submaximal exercise capacity to participate in low to moderate-intensity activity and active play with peers, potentially enabling the health benefits of an active lifestyle. Nonetheless, the current data should not be extrapolated to all children with cardiomyopathy. Rather, these data point to a compelling need for more explorations in the area of physical activity participation to capture a larger and more diverse sample of children with cardiomyopathy.
Acknowledgements
Acknowledgements: The support of participating families and contributions of the cardiology clinic staff, specifically, Denise Melo and Tyler Kung, for assistance during exercise study assessments, is greatly appreciated. This study was made possible by the support of Barb Kennedy and the project coordination of John Sawdon from the Cardiac Health Foundation of Canada.
Notes
Financial Support
This research was funded by the Ontario Trillium Foundation (Grant number: SD99638). KM was supported by a University of Ottawa Graduate Student Scholarship and by the Ontario Trillium Foundation.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Standards
Ethics approval and consent to participate were obtained from the Children’s Hospital of Eastern Ontario Research Ethics Board (REB study #17/189x) and the University of Ottawa (H-04-18-461). All procedures contributing to this work complied with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.